The time when everyone dumped on Andrew Wakefield, but looked the other way while pro-vaccine researchers & officials engaged in blatant shitefookery.

Note: This is a long article, and I get that for some people it won’t be as instantly enthralling as reading about the latest Trump sex scandal. However, if you truly wish to make sense of the ‘research’ claiming no link between autism and vaccines, I strongly urge you to read this article in its entirety. Brew a cup of tea, read it in installments, whatever, but make it through to the end and you will be much wiser to the statistical chicanery used by pro-vaccine researchers and government agencies. You’ll also get an enlightening insight into the moral and intellectual - and sometimes outright criminal - character of these researchers and agencies.
What I’m going to discuss today occurred over 20 years ago, but I’ve personally seen no mention of it here on Substack. It involves two scientific papers that lucidly illustrate both the egregious dishonesty and raging hypocrisy that dominates the pro-vaccine juggernaut.
Our discussion today centers around these supposedly peer-reviewed papers, most notably an article published in September 2003 by the prominent medical journal Pediatrics. The article is titled “Thimerosal and the Occurrence of Autism: Negative Ecological Evidence From Danish Population-Based Data”.
The researchers explicitly declared “Our ecological data do not support a correlation between thimerosal-containing vaccines and the incidence of autism.” (Bold emphasis added)
As you’re about to learn, this is simply not true.
That, of course, didn’t stop the paper’s conclusion being incessantly cited by the mainstream media.
The lead author on the 2003 pro-vaccine paper was one Kreesten Meldgaard Madsen. This was actually the second pro-vaccine paper on which Madsen was listed as lead author; the first was a 2002 New England Journal of Medicine paper titled “A Population-Based Study of Measles, Mumps, and Rubella Vaccination and Autism”.
Neither the Pediatrics nor NEJM paper contains any disclosure or conflict of interest section. The NEJM paper, however, reveals that study was funded by grants from several outfits, not least of which was the US Centers for Disease Control and Prevention (CDC).
We’ll come back to this later.
There is very little information about Madsen on the Internet, which is somewhat curious for a guy whose work has been cited incessantly to discredit any link between mercury-containing vaccines and autism.
The 2002 and 2003 papers list Madsen as hailing from the Department of Epidemiology and Social Medicine, University of Aarhus, Denmark.
Madsen’s educational qualifications, reported from a since-removed webpage, are:
Student clinical neurology and pediatrics, University Oxford, United Kingdom, 1994.
Doctor of Medicine, University Aarhus, Denmark, 1996.
Diploma of medical research, University Aarhus, Denmark, 1996.
Doctor of Philosophy in Epidemiology, University Aarhus, Denmark, 2004.
I’ll ask you to note there is nothing in his qualifications pertaining to pharmacology, dermatology or drug development. The reason why will become obvious shortly.
It seems Madsen published his two epidemiological pro-vaccine papers while still a student of epidemiology. It’s not unheard of for PhD students to collaborate on a published paper with a senior professor, who then allows their younger protege’s name to take pole position on the paper (this very favor was afforded to one Dr Robert Malone, his constant whining about being an under-recognized pioneer notwithstanding).
However, the NEJM and Pediatrics papers each feature 6-7 additional co-authors. Given the numerous other supposed epidemiologists listed alongside Madsen, it does seem unusual for someone who hasn’t yet completed their PhD to be awarded lead author status.
It would make sense, however, if it turns out Madsen was being groomed by actors with an interest in discrediting the vaccine-autism link.
Big Pharma has a highly effective ongoing operation known as the “Key Opinion Leaders” sham. KOLs are supposedly experts in the field that graciously share their knowledge with other medical practitioners. In reality, the true purpose of KOLs is “influencing the prescription behaviour of practitioners … with the main purpose of enhancing and perpetuating profit rather than innovation and critical thinking.”
The beauty of the KOL charade, from the perspective of drug companies, is that you can pretty much take any nondescript, non-outstanding individual with a medical or scientific qualification and turn them into an overnight ‘expert’. You just need them to be amenable to a little palm-greasing and/or promises of enhanced career prestige. They then agree to lend their name to a ghost-written paper, even if they don’t fully comprehend the paper’s contents. Not to worry: The very act of authoring a peer-reviewed paper, especially in a big name journal, automatically endows them with a degree of respect and credibility they would otherwise not enjoy.
After bursting on to the published paper scene with two pivotal papers, Madsen seems to have largely stayed out of the public limelight.
However, thanks to this 2023 press release, we know Madsen was appointed that year as Chief Development Officer at LEO Pharma, a Danish drug company where he has worked since 2016.
This, apparently, wasn’t Madsen’s first drug development rodeo; he allegedly came to LEO Pharma “with broad leadership and drug development experience from a number of R&D organizations.” Prior to snagging the CDO spot, he was LEO’s “Head of R&D, Asia Pacific Hub.”
LEO Pharma’s focus is on “therapies for the treatment of skin diseases, such as psoriasis, Chronic Hand Eczema (CHE), atopic dermatitis, acne and infections”.
So the next question is why was a regular medical doctor and epidemiologist appointed head of R&D at a company that makes dermatological drugs, and how has he established “broad leadership” in “drug development”?
Would it be for the same reason that a stripper with no science or medical qualifications was made Regional Sales Director at a drug company later ensnared in a fentanyl scandal?
Namely, that these people are often appointed based on marketing and business considerations, rather than their scientific aptitude?
The LEO press release claims Madsen has “a long list of scientific publications with more than 4,000 citations in international publications.”
What a complete crock.
A Pubmed search for “Madsen KM” returns only 111 results, and not one of them has to do with skin disorders or dermatology drugs. Furthermore, most of those papers are not even authored by Kreesten, but by American Kirsten M Madsen, who was evidently a prolific nephrology researcher.
Madsen’s role in this charade is already looking rather curious, and we haven’t even looked at his actual papers yet.
How to Massage ‘Adjust’ the Data to Get the Results You Want
The 2002 NEJM paper reported on 537,303 Denmark children of which 82% had received the MMR vaccine.
They claimed an 8% lower relative risk of autistic disorder in the vaccinated group as compared to unvaccinated children. Madsen et al thusly concluded, "This study provides strong evidence against the hypothesis that MMR vaccination causes autism."
Like hell it does.
Before we even get to the results, we already see a problem with the study methods, which included “all children born in Denmark during the period from January 1, 1991, to December 31, 1998.”
We then learn that the end of follow-up occurred “on December 31, 1999”.
That is a major problem because a systematic review of the research found a mean age for autism diagnosis of 60.48 months (just over 5 years of age).
Indeed, from their own data, Madsen et al reported “The mean age at diagnosis was four years and three months for autistic disorder and five years and three months for other autistic-spectrum disorders.”
So their own methods and data confirm that many of the children in their sample - those born circa 1994 onwards - were too young to have been diagnosed with autism, meaning the true number of autistic children was almost certainly underrepresented.
But that’s hardly the end of it.
There are a myriad of ways to interpret and present the same data, and in studies sponsored by vested interests, the preferred method is whichever one delivers the most-favorable-looking results.
Madsen et al present their results based on person-years, for which they then ultimately derive an “adjusted relative risk”.
They declare adjusted relative risks for “autistic disorder” and “other autistic-spectrum disorders” of 0.92 and 0.83, respectively. Anything below 1.0 indicates a reduced risk, so what the authors are claiming is that vaccination was associated with a slightly decreased risk of these disorders.
In Table 2 of their 2002 paper, Madsen et al present the total person years and RRs for the following categories: “Age at vaccination,” “Interval since vaccination”, and “Date of vaccination”.
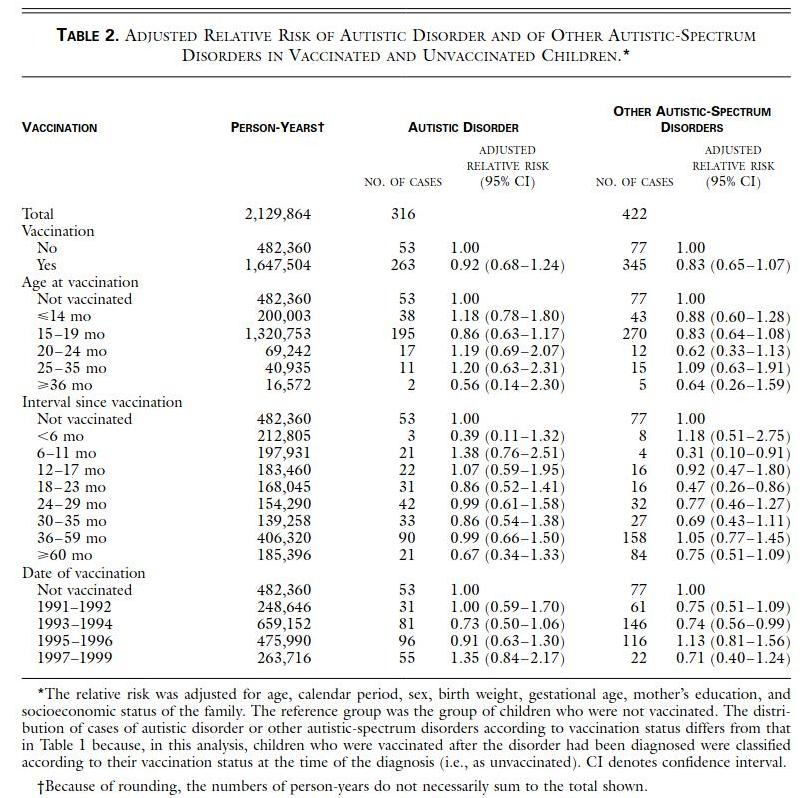
In the “Age at vaccination” category, we can see that three of the five vaccination age categories actually show increased adjusted risks for autism disorder, ranging from 1.18 to 1.20.
However, the results are swayed by the 15-19 month category, which features a wildly disproportionate number of person years (1,320,753), and an accompanying RR of 0.86. The other category showing a reduced RR was >36 mo, which featured a vastly lower number of person-years.
So we have a study where the two favorable RRs occur in groups with disproportionately large and small portions of the total cohort.
That study featured up to 8 years of follow-up, yet its “Age at vaccination” analysis is dominated by the 15–19 month category. Why would this category show a lower risk of autism when most others showed increased risks? Is there something magical about getting vaccinated at 15-19 months that protects against autism?
If there is not, it would mean the results are a crock.
I’m unaware of any plausible biological mechanism that would explain this paradox, so I’m detecting the pungent aroma of mierda del toro here. It turns out Dr. Samy Suissa, from the Department of Epidemiology and Statistics at McGill University, also found the figures a bit stinky.
If you take a look at Table 2 above, you’ll see Madsen et al have presented the overall numbers of person-years and the corresponding number of autism and “other” cases. What they do not do is present the rates in terms of per 100,000 person-years, which would provide a standardized rate that would then make it much easier to place the data in their correct context. The standardized rates derived from the per 100,000 person-years calculations would be known as the “crude” (unadjusted) incidence rates.
Instead they only present the relative risk figures that have been adjusted for a small number of countless potential confounders, listed in fine print at the bottom of the table.
When we calculate crude per 100,000 person-years figures for the “Age at vaccination” category, as Dr Suissa did, we observe something very interesting. Check it out:
Not vaccinated: 10.98 cases
<14 mo: 18.99 cases
15–19 mo: 14.76 cases
20–24 mo: 24.55 cases
25–35 mo: 26.87 cases
>36 mo: 12.06 cases
So now a very different picture emerges. Every single age category of vaccinated children has a notably higher rate of autistic disorder diagnoses than the unvaccinated category. That includes the 15-19 month and >36 month categories that were massaged into showing reduced relative risks during the ‘adjustment’ process.
For the 15-19 month and >36 month figures to look so different after adjustment, one or more of the factors for which ‘adjustment’ took place must have had a major impact. But which one/s? And by what mechanism/s?
Just which of “calendar period, sex, birth weight, gestational age, mother’s education, and socioeconomic status of the family” allegedly impacted the unvaccinated category so dramatically?
And why?
You can’t just present curious results like this and then act like nothing ever happened. But that’s exactly what Madsen et al do. Not only that, but to prevent most readers from ever identifying the discrepancies between the crude and adjusted figures, they avoid presenting the person-years data in “per 100,000” format, as is standard practice in papers featuring this metric.
By the way, Dr Suissa penned a letter to the New World Order England Journal of Medicine outlining these highly pertinent concerns.
They declined to publish it.
Okay, so what we’ve observed so far reeks of shady research practice, but it’s by no means smoking gun proof of fraud.
So, my friends, I would like to now discuss the Masden et al 2003 Pediatrics paper.
When Your Data Shows One Thing, and You Brazenly Claim the Opposite
In the Pediatrics paper, Madsen et al purportedly set out to examine “whether discontinuing the use of thimerosal-containing vaccines in Denmark led to a decrease in the incidence of autism.”
Surprise, surprise, they found “discontinuation of thimerosal-containing vaccines in Denmark in 1992 was followed by an increase in the incidence of autism.” (Bold emphasis added).
So they were not only concluding there was no correlation between thimerosal-containing vaccines and autism, but that injections containing a neurotoxic heavy metal were in fact protective against this neurological disorder.
Sure thing.
According to Dr Brian Hooker, “This paper has two severe methodological flaws. First, the Denmark NCRR database changed diagnostic criteria for autism diagnoses in 1994 from ICD8 to ICD10. This led to a greater number of autism diagnoses overall.”
“Second, the Denmark NCRR database changed the accounting of autism based on outpatient visits in 1995, whereas up to 1995, only inpatient (i.e., Hospital) visits were accounted. This led to a significant increase in autism cases counted beyond 1994.”
“These two data artifacts … show a misleading jump in the prevalence of autism after 1995. However, when these are corrected for, the actual autism rates in Denmark decreased by as much as 4 times upon the phase out of thimerosal-containing vaccines (Trelka et al. 2004).”
“Although the raw data from the Madsen et al. 2003 publication has been requested, the authors chose not to release it, creating significant difficulty in confirming this decrease.”
What are you hiding, Kreesten?
A recent review that documented increasing prevalence of autism in Scandinavian and Nordic countries discusses possible contributors such as “heightened awareness of ASD and earlier diagnosis.” Nowhere does it mention the elimination of toxic compounds being injected into children as a reason for the increase.
That review also notes that, for diagnosis of autism spectrum disorder, Denmark used ICD-8 from 1987 to 1993, leap-frogging to ICD-10 from 1994. Hence, ICD-9 was never implemented in Denmark. So there was indeed a marked change in the criteria for diagnosing autism in Denmark beginning 1994.
And Madsen et al knew it.
FOI documents obtained from the CDC clearly indicate the 2003 paper omitted data showing autism rates actually dropping after mercury was removed from Danish vaccines.
One coauthor from Aarhus University, Denmark, whose name has been redacted, was aware of the omission and stated in a 2002 email to the CDC, "Attached I send you the short and long manuscript about Thimerosal and autism in Denmark ... I need to tell you that the figures do not include the latest data from 2001 ... but the incidence and prevalence are still decreasing in 2001" (Bold emphasis added).
{kind=link}
Madsen et al used 2000 as the cut-off year for follow-up in their 2003 paper.
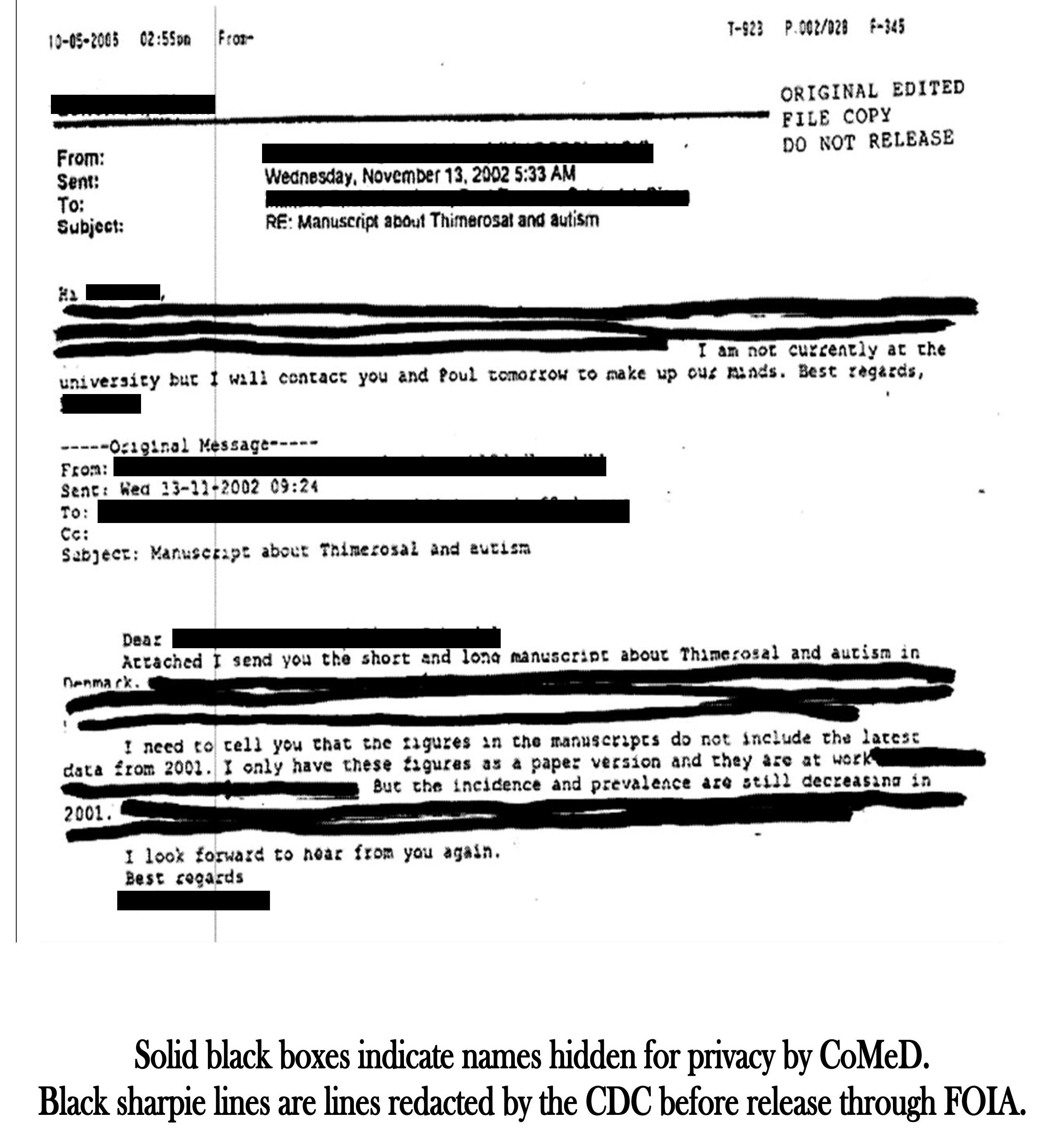
According to the Coalition for Mercury-Free Drugs, it is Madsen who replies: "I am not currently at the university but I will contact you and Poul tomorrow to make up our minds."
As you’ve probably surmised, in the final draft version of the publication submitted to Pediatrics, the inconvenient data from 2001 showing a decline in autism was not mentioned.
Despite this, the CDC endorsed the article and, in a December 10, 2002 recommendation letter to the editor of Pediatrics, encouraged expedited review and publication of the article.
How Madsen et al Hid the Inconvenient Truth
Commonsense dictates that removing a neurotoxic compound like mercury from the vaccine schedule would lead to a lower rate of neurological disorders like autism.
Here’s exactly how Madsen and his accomplices maneuvered to hide that decline.
We know that in 1992, thimerosal was removed from childhood vaccines in Denmark.
We also know that in 1994 Denmark adopted the ICD-10 criteria for diagnosing autism (“ICD”, by the way, stands for the WHO’s International Classification of Diseases, which are periodically updated).
Denmark previously used ICD-8, and never adopted ICD-9.
This is critical because there was no actual mention of "autism" in ICD-8. Instead, the category of "299 Unspecified psychosis" was used.
It wasn't until ICD-9 that "299 Infantile autism" was added.
ICD-10 expanded the criteria and added further diagnoses like "Asperger syndrome", "childhood autism", "atypical autism" etc.
This meant far more children were eligible to be diagnosed with autism and related disorders.
Which, of course, would have served to mask a decline in actual autism rates.
To truly determine whether the rate of autism had gone down after 1994, you'd need to set aside the ICD codes and apply a consistent set of diagnostic criteria for "autism" across the entire follow-up period.
That would likely be impossible because it would require examining the case notes of all the kids diagnosed with autism during that follow-up period.
Madsen et al, needless to say, did not do this. Instead, the methods section of their paper confirms they used ICD-8 for the pre-1994 period, and ICD-10 for 1994 onwards.
That right there is a massive flaw, because they are comparing apples with oranges.
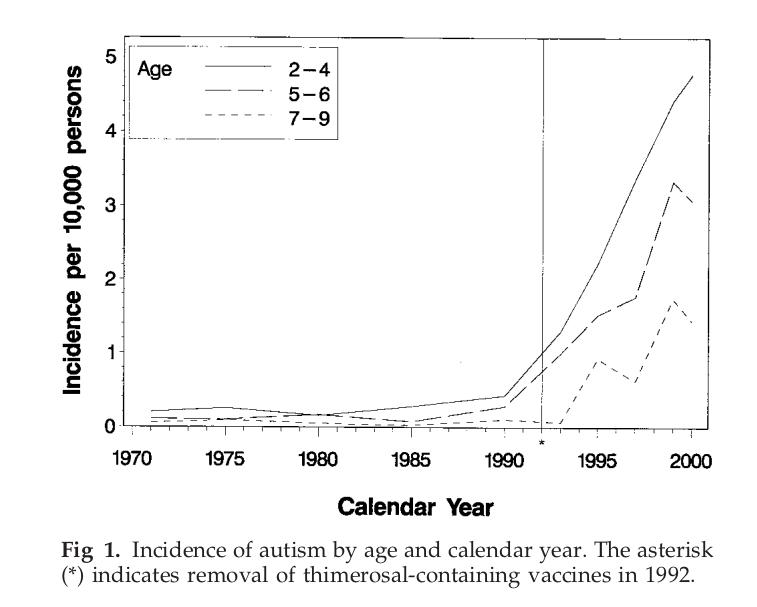
But then something interesting happens. Even with the new expanded criteria, the incidence of autism starts to decline in Denmark by the late 1990s!
This corresponds with the time lag you would expect if thimerosal caused autism, because, as noted, the mean age of diagnosis is around 5 years of age.
The decline is clearly visible in Fig. 1 of the 2003 Pediatrics paper. By 1999, the trajectories for the 5-9 age groups have peaked and begun a clear decline.
The FOI-obtained email reprinted above confirms Madsen et al had data for 2001 that showed this decline was continuing, but they deliberately left it out of the paper. That email was also sent to the CDC, who similarly ignored it. I’ve explained previously that the CDC is a hopelessly dishonest vaccine business masquerading as a public health agency.
The only feasible reason for deliberately omitting the post-2000 data is because it would have amplified the downward trajectory evident from 1999 onwards. Allowing readers to view that continuing downward trajectory was not in keeping with what was clearly a preconceived agenda to absolve thimerosal-containing vaccines of any role in autism.
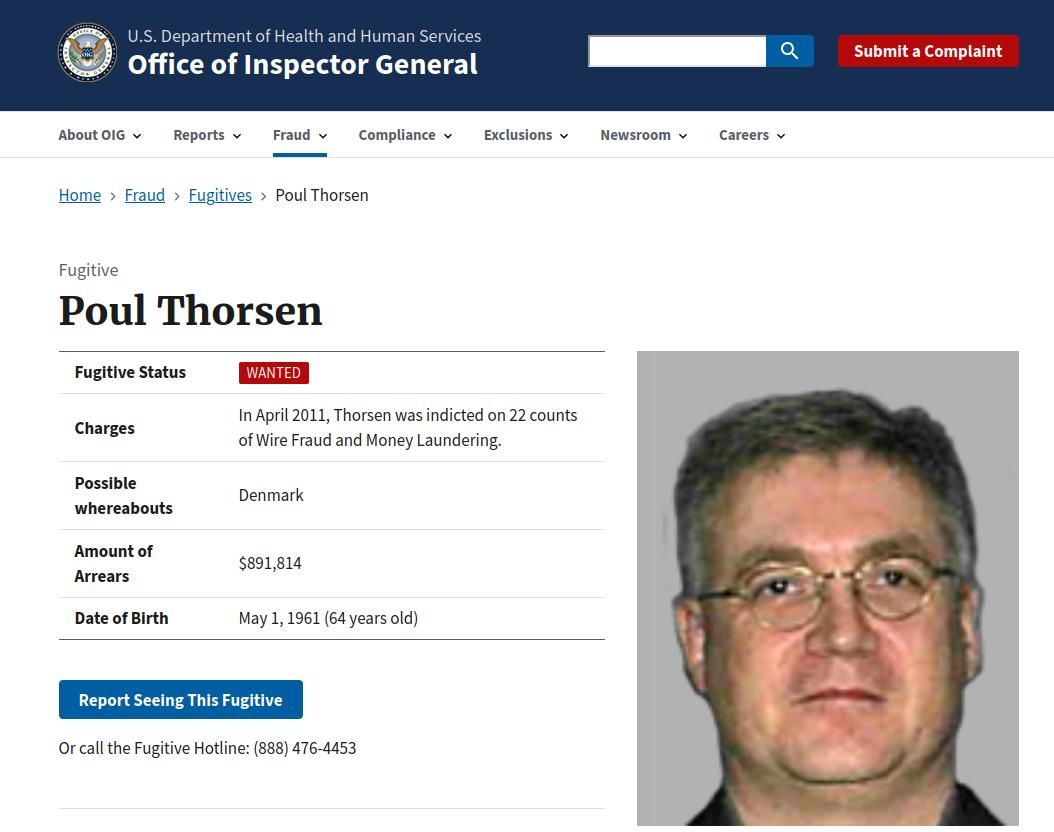
Madsen’s Fugitive Co-Author
The “Poul” that Madsen refers to in the above email exchange is Dr. Poul Thorsen, a co-author of the NEJM and Pediatrics papers and, by way of remarkable coincidence, "scientist in residence" at the CDC during 2000-2002.
To call Thorsen a shifty bastard would be an understatement. Aarhus University emphatically distanced itself from him in 2010 after “a considerable shortfall in funding at Aarhus University associated with the CDC grant was discovered.”
The following year, Thorsen was criminally indicted in Atlanta for embezzlement in relation to $11 million worth of CDC grants.
It was alleged Thorsen had diverted at least $1 million of this taxpayer money to distinctly non-research activities, including the purchase of “a home in Atlanta, a Harley Davidson motorcycle, and Audi and Honda vehicles.”
In response, Thorsen fled the US. He remains on the HHS-OIG wanted list as a fugitive.
Rules For Thee, Not For Me!
During the Great Covid Con, journals were retracting papers left, right and center. Deficient and disingenuous reasoning was sometimes given, but usually no reason of substance was provided at all. The journals simply wanked on about unspecified “concerns” with the paper’s methods and conclusions, which was code for:
“We’ve been tapped on the shoulder and firmly reminded we are not to publish anything that goes against the official narrative. Otherwise unpleasant circumstances may befall us.”
The 2002 and 2003 Madsen et al papers came shortly after the infamous 1998 Wakefield et al paper. Andrew Wakefield was subsequently crucified for that retracted paper, and to this day any mention of his name by the mainstream media and the “Mercury is Good For You!” crowd are inevitably accompanied by the word “disgrace”.
This is despite the fact that Andrew Wakefield absolutely did not do any of the things he was accused of.
The only fraudulent things about Andrew Wakefield are his accusers and critics.
Meanwhile, two papers with clearly garbage and highly suspicious methodology that were used to defend mercury-containing vaccines have not been retracted from the prominent journals in which they were published.
This is despite obvious and serious flaws, and an email showing the authors admitting one of their papers omitted inconvenient data, and one of the co-authors now being an on-the-run fugitive!
Honest researchers don’t fudge their data, and they do not deliberately omit relevant stats.
They don’t need to.
When the authors of prominent pro-vaccine papers have to employ such methods to portray thimerosal-containing vaccines as safe, it’s wise to assume they are not.
Note: Article updated 28 August 2025 to include Fig. 1 from the 2003 Pediatrics paper and further elucidate how Madsen et al hid the post-2000 decline in autism diagnoses.
Leave a Reply