The biggest corporate criminal in US legal history now being sued for selling its popular contraceptive without warning users of the risk.
I recently wrote about the growing volume of case studies reporting “turbo cancers” appearing shortly after COVID ‘vaccinations’. As marketer of the chart-topping clot shot BNT162b2 aka Cominarty, Pfizer is a major contributor to the turbo cancer phenomenon.
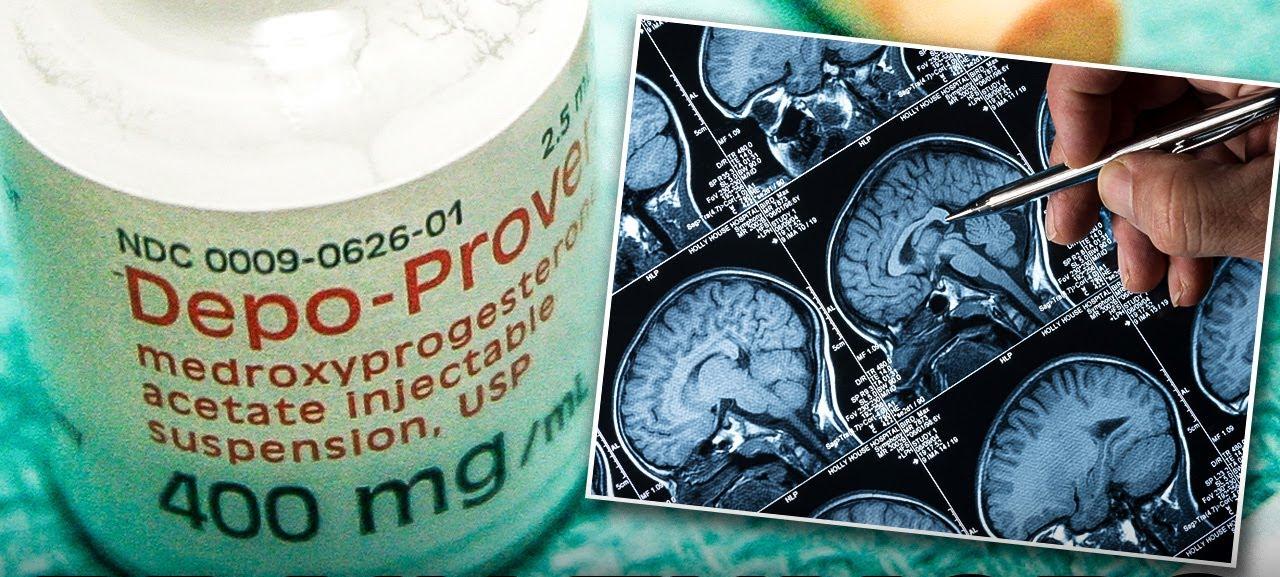
Cominarty is hardly the only Pfizer drug that increases risk of developing dangerous growths inside the body. Last year, a study found Pfizer’s widely-used contraceptive Depo-Provera (medroxyprogesterone acetate) greatly increases risk of meningiomas, tumors that form on membranes covering the brain and spinal cord just inside the skull.
Meningiomas are mostly slow-growing benign tumors but can nevertheless compress adjacent brain tissue and thus patients may require surgical decompression. The incidence of meningiomas increases with age, rising sharply after the age of 65 years.
Pfizer knew Depo-Provera increased the risk of meningiomas, but failed to warn US physicians and users. This now forms the cornerstone of a massive lawsuit against the company, launched on behalf of US women who developed meningiomas after receiving at least 4 consecutive injections of the drug. One of the firms overseeing the multidistrict litigation is Levin Papantonio, which has helped to secure more than $80 billion in jury verdicts and settlements against some of the world's largest corporations, including Johnson & Johnson, BP, Dupont, 3M, Merck and big tobacco. The law firm is currently acting for plaintiffs in the Talcum Powder Litigation against Johnson & Johnson, the darlings who sold us asbestos-laced baby powder for years on end.
The lawsuits allege Pfizer and other generic producers of Depo-Provera were aware of the link between the injections and brain tumors yet failed to adequately warn of the risk and promote safer alternatives. Pfizer added warning labels in Canada in 2015, and in the UK and Europe in October 2024, following a study published in the British Medical Journal. On February 25, 2025, Pfizer issued a note to healthcare professionals in South Africa warning the drug can cause meningiomas and should not be used by patients with a history of the condition. However, Pfizer has never provided an equivalent warning in the lucrative United States market.
Pfizer is attempting to have the lawsuit thrown out, arguing it cannot be sued under state failure-to-warn laws because its corrupt and secretive buddies at the FDA previously rejected a proposed warning about the risk of brain tumors on the Depo-Provera label. Pfizer’s liars-for-hire are arguing federal law preempts any state claim requiring a warning the FDA refused to approve.
Pfizer, in other words, is not arguing the drug is safe nor denying a warning label would have been beneficial for users. It is simply arguing it’s not legally culpable because its friends at the industry-funded and -bribed FDA, with whom Pfizer has an enduring revolving door arrangement, inexplicably nixed calls for a warning label.

The BMJ study was published in March 2024. It was a case-control study with 18,061 women in France who had intracranial surgery for meningioma between January 1, 2009 and December 31, 2018. Each of these cases was matched to five controls for year of birth and area of residence (90,305 controls).
The mean age of all women was 57.6 years. Most meningioma cases were benign (92.3%), while 5.8% were classified as atypical and 1.9% as malignant. Mortality was higher among cases than controls: 2.8% of cases died within two years versus 1.2% of controls, while 5.3% died within five years versus 3.4% of controls. Mortality, not surprisingly, was higher for the cases with malignant tumors, 12.5% of whom died within two years and 20.7% within five.
The analysis found excess odds ratios for meningioma for several progestin-based contraceptives:
Cyproterone acetate: OR 19.21
Medroxyprogesterone acetate (Depo-Provera): OR 5.55
Nomegestrol acetate: OR 4.93
Chlormadinone acetate: OR 3.87
Medrogestone: OR 3.49
Promegestone: OR 2.39
This excess risk was driven by prolonged use (≥one year). Three quarters of the women in the cases group exposed for more than a year had in fact been exposed for more than three years.
The analysis detected no excess risk of intracranial meningioma for progesterone, dydrogesterone, or levonorgestrel intrauterine systems.
No conclusions could be drawn concerning dienogest or hydroxyprogesterone because of the small number of individuals who received these drugs.
Taking Synthetic Hormones Your Body Doesn’t Need, and You Know Nothing About, For Years on End: What Could Possibly Go Wrong?
I’ve long marveled at the difference in societal attitudes towards use of sex hormones by women and men. Use of testosterone and the hormone analogs falling under the banner of “anabolic steroids” by males has long been the subject of often hysterical press coverage.
Meanwhile, few bat an eyelid over decades-long use of estrogens and progestins by women, even though such use has long been linked to several adverse and serious health outcomes.
Irrespective of whether you pee standing up or sitting down, messing with your body’s hormones is not something to be taken lightly. Yet for decades now, doctors have handed out hormone-based contraceptives to women as if they were candy. We owe this bizarre situation in no small part to the globalist-funded brain cancer known as ‘feminism’, a distinctly anti-feminine ideology that convinced women around the world consequence-free sex was a birthright.
There’s no such thing as a free lunch, folks, not in nature and not in the urban jungle.
Reading through the online product information for Depo-Provera leaves one to marvel at just how this junk became so popular.
“[L]oss of bone mineral density (BMD) may occur in pre-menopausal women who use [medroxyprogesterone acetate] injection long-term” (p 1)
“Use of MPA injection reduces serum estrogen levels in premenopausal women and is associated with a statistically significant loss of BMD as bone metabolism accommodates to a lower estrogen level. Bone loss may be greater with increasing duration of use and may not be completely reversible in some women.” (p 4)
“There was a tendency for women to gain weight while on therapy with MPA.” (p 6)
“Two large clinical trials [WHI CEE/MPA and HERS] showed a possible increased risk of cardiovascular morbidity in the first year of use and no overall benefit” with combined combined conjugated estrogen and medroxyprogesterone acetate use. “In the WHI CEE/MPA trial, an increased risk of coronary heart disease (CHD) events … was observed in women receiving CEE/MPA compared to women receiving placebo (37 vs. 30 per 10,000 person years). The increase in VTE risk was observed in year one and persisted over the observation period.” (p 7)
“In the WHI CEE/MPA trial, an increased risk of stroke was observed in women receiving CEE/MPA compared to women receiving placebo (29 vs. 21 per 10,000 person-years). The increase in risk was observed in year one and persisted over the observation period.” (p 8)
“In the WHI CEE/MPA trial, a 2-fold greater rate of VTE, including deep venous thrombosis and pulmonary embolism was observed in women receiving CEE/MPA compared to women receiving placebo. The increase in risk was observed in year one and persisted over the observation period.” (p 8)
“The Women’s Health Initiative Memory Study … an ancillary study of WHI, CEE/MPA reported an increased risk of developing probable dementia and mild cognitive impairment (MCI) in post-menopausal women 65 years of age or older.” (p 8)
“MPA may produce Cushingoid symptoms … Some patients receiving MPA may exhibit suppressed adrenal function. MPA may decrease ACTH and hydrocortisone blood levels.” (p 9)
“Some reports suggest an association between intrauterine exposure to progestational drugs in the first trimester of pregnancy and genital abnormalities in fetuses. Infants from unintentional pregnancies that occur 1 to 2 months after injection of MPA injectable suspension may be at an increased risk of low birth weight, which, in turn, is associated with an increased risk of neonatal death.” (p 10)
Among “clinical studies that enrolled more than 4200 women who received MPA for contraception for up to 7 years” the most frequently reported adverse drug reactions were “weight increase (69%), weight decrease (25%), headache (16%), nervousness (11%), abdominal pain or discomfort (11%), dizziness (6%), and decrease in libido (6%).” (p 10)
In “Phase 3 clinical studies that evaluated efficacy and safety of MPA in gynecology” the most frequently reported adverse drug reactions were “dysfunctional uterine bleeding (19%), headache (12%), and nausea (10%).” (p 11)
“Long-term intramuscular administration of medroxyprogesterone acetate (MPA) has been shown to produce mammary tumors in beagle dogs.” (p 19)
“Meningiomas have been reported following long term administration of progestins, including MPA. MPA should be discontinued if a meningioma is diagnosed. Caution is advised when recommending medroxyprogesterone to patients with a history of meningioma.” (p 4)
The most recent FDA-approved package insert for Depo-Provera of course makes no mention of the increased meningioma risk.
It does admit 3 of 5 large case-control studies found “a slightly increased risk of breast cancer in the overall population of users; these increased risks were statistically significant in one study. One recent US study evaluated the recency and duration of use and found a statistically significantly increased risk of breast cancer in recent users (defined as last use within the past five years) who used DMPA for 12 months or longer; this is consistent with results of a previous study.” (s 5.3)
“Most women using Depo-Provera CI experience disruption of menstrual bleeding patterns. Altered menstrual bleeding patterns include amenorrhea, irregular or unpredictable bleeding or spotting, prolonged spotting or bleeding, and heavy bleeding.”
With longer term use, “fewer experience irregular bleeding and more experience amenorrhea. In clinical studies of Depo-Provera CI, by month 12 amenorrhea was reported by 55% of women, and by month 24, amenorrhea was reported by 68% of women using Depo-Provera CI.” (s 5.10)

Leave a Reply