
In April last year, as lockdown totalitarianism kicked into high gear, media outlets gave brief mention to a study about the potential for vitamin D to reduce the risk of influenza and COVID-19. Titled "Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths," the paper's head author was long-time vitamin D researcher William B. Grant.
Since then, vitamin D has been largely ignored by the media and our dishonest authorities, who have instead embraced a "vaccine or bust" propaganda campaign. This PR campaign has positioned vaccination as the only hope for civilization - the only possible protection against the not-so-deadly COVID-19, which studies repeatedly show has an infection fatality rate of less than 0.5%.
Vitamin D already exists, and is a cheap, non-patented and readily available vitamin. And, as clinical trials have repeatedly demonstrated, it's safe.
But because it's not a man-made, patentable chemical, vitamin D offers little profit potential for drug companies and the numerous wealthy and influential people who are heavily invested in these companies - nor the researchers who receive money from them, the media outlets who enjoy revenue from pharmaceutical advertising, and the countless politicians and bureaucrats who are the subject of intense drug company lobbying.
Here are but a few examples of the pervasive conflicts of interest in the COVID-19 vaccine campaign:
- After being caustically (and, as it turns out, unfairly) ridiculed for talking up hydroxychloroquine, President Donald Trump folded and embraced the vaccine charade. In May last year he appointed Moncef Slaoui to lead "Operation Warp Speed," the federal administration initiative to accelerate the discovery of a COVID vaccine. In keeping with the time-honoured "revolving door" phenomenon, Slaoui was on the board of directors at Moderna before he took on the Warp job. Slaoui is also a former head of vaccine development at pharmaceutical giant and serial lawbreaker GlaxoSmithKline. SEC filings showed Slaoui still held more than 150,000 stock options in Moderna, worth over $10 million, at the time of his appointment. And that was before the company's stock price shot up after reporting 'promising' early results from its vaccine testing.
- Earlier this year, a research collaboration between Moderna and researchers at Anthony Fauci's National Institute of Allergy and Infectious Diseases revealed several of the latter "are inventors on US Patent Application No. 62/972,886 227 entitled '2019-nCoV Vaccine.'" These vested researchers were Kizzmekia S. Corbett, Olubukola M. Abiona, Geoffrey B. Hutchinson and Barney S. Graham, all hailing from the NIAID's Vaccine Research Center in Bethesda, Maryland. So-called fact check (i.e. Thought Police) websites like The Dispatch expect us to be reassured by the fact that "While these four NIH scientists may receive royalties from the vaccine, federal law prevents their compensation from exceeding $150,000 a year." Considering $150,000 in the US can buy a brand new Porsche for you and another for the missus, I'm not at all reassured. The Dispatch also makes no mention that these are exactly the kind of researchers likely to find themselves even higher-paying positions in Big Pharma as a thank you for their 'co-operation' while working at an influential federal government agency.
- Shares of German company CureVac recently surged on the news it was partnering with Bayer to develop its COVID vaccine. The company’s second-largest shareholder (behind German billionaire Dietmar Hopp) is the Bill and Melinda Gates Foundation, which has pumped over $44.2 million into CureVac.
The Gates Foundation is also heavily in invested in BioNTech, a publicly-traded German company collaborating with Pfizer on a COVID vaccine, Pfizer, and Vir Biotechnology, which has partnered with GlaxoSmithKline to develop an antibody therapy targeting COVID-19.
Bill Gates is a high school dropout who became the world's richest man by selling bloated, buggy computer software. This, apparently, qualifies him as a public health expert. Gates is a long-time proponent of global population reduction, and harbors a fetish-like obsession with vaccines. At TED2010, Gates lamented to his audience that the world population was 6.8 billion and "headed up to about 9 billion." But, he added, "If we do a really great job on new vaccines, health care, reproductive health services, we could perhaps lower that by 10 or 15%."
Given that the entire premise underpinning vaccination is that it saves lives, one cannot help but wonder why Bill Gates is convinced new vaccines will help reduce the world's population by 10-15% ... ?
 Vaccines are so good at saving lives, says Bill Gates, that he believes they can help reduce the world's population by 10-15%.
Vaccines are so good at saving lives, says Bill Gates, that he believes they can help reduce the world's population by 10-15%.
Huge fortunes are being made in the COVID vaccine charade, even in companies who have yet to bring a tested vaccine to market. Humble vitamins like vitamin D, meanwhile, aren't going to make anyone rich. Vitamin D is not the subject of multi-million dollar government grants nor is it the subject of wild, skyward share price spikes. A year's supply of vitamin D, at the daily dose of 5,000 IU, costs less than $14 per year.
The Evidence for Vitamin D
Before we discuss the effect of vitamin D on COVID, let's take a look at why vitamin D should be a regular part of your supplement arsenal, scamdemic or no scamdemic. Numerous meta-analyses of randomized controlled trials have found vitamin D supplementation protects against respiratory tract infections[1-3].
The most recent of these, published in BMJ (British Medical Journal) in 2017, analyzed 25 clinical trials with some 11,000 participants. Among all these participants combined, vitamin D supplementation reduced the risk of acute respiratory tract infection among all participants by 12%. The risk reduction was greater in those receiving daily or weekly vitamin D (-19%) compared to those receiving larger but infrequent 'bolus' doses of at least 30,000 IU (-3%).
At first glance, a risk reduction of 12-19% may not seem that spectacular, but this is where Captain Obvious arrives to save the day:
Supplemental vitamin D will provide the most benefit to those who are most vitamin D-deficient.
Duh.
And so when the researchers further analyzed the results according to baseline serum 25-hydroxyvitamin D (25(OH)D) levels, the results suddenly became far more newsworthy.
Among those receiving daily or weekly vitamin D, protective effects were far stronger in those with baseline 25-hydroxyvitamin D levels below 25 nmol/L. In this group, the incidence of acute respiratory tract infection was 70% less than in the control group.
In those with baseline 25-hydroxyvitamin D levels ≥25 nmol/L, the incidence of acute respiratory tract infection was reduced by 25%.
The most definitive outcome when looking at clinical trials is death. Little risk of misdiagnosis there, unless the doctor has screwed up spectacularly (while rare, it does happen). However, no separate figures for death rates according to baseline serum vitamin D status was presented, probably because the numbers were too small for any meaningful analysis. In the overall sample, there was no difference in death rates from ARI, any infection or any cause between vitamin D and control subjects - not surprising given the small effect of vitamin D on ARIs in the overall sample.
So what about COVID?
So far, there have been very few trials published that specifically examine the effect of vitamin D on COVID incidence and outcomes. In fact, I have only been able to locate two small trials in the English-language literature.
The first to be published was a study involving all consecutive COVID-19 patients aged 50 years and over admitted to Singapore General Hospital between 15 January and 15 April 2020. As the COVID- 19 situation evolved, the researchers decided from 6 April 2020 to start supplementation on all COVID-19 patients above 50 years old if they did not require oxygen therapy. Similar patients admitted before this date did not receive the supplement and therefore served as the control population. The supplement therapy comprised a single daily oral dose of vitamin D3 1,000 IU, magnesium 150mg and vitamin B12 500mcg for up to 14 days. These were quite modest dosages.
Significantly fewer patients receiving the vitamin D/magnesium/B12 combination suffered clinical deterioration. Only 3 of 17 patients receiving the supplements required subsequent oxygen therapy, compared to 16 of the 26 controls. Only 1 of the 17 supplemented patients required ICU support, compared to 8 of the 26 control patients.
No patients died in either group.
There are a few caveats. It was obviously a small study and was not randomized nor blinded. The patients receiving the supplement combo were on average over 5 years younger and were less likely to have hypertension. However, multivariate analysis showed the supplements remained a significant protective factor against clinical deterioration after adjusting for age or hypertension separately. I'm rather wary of the whole statistical 'adjustment' caper, but the researchers also did another sub-analysis where they excluded patients under 60. This smaller sample of 20 had near-identical ages (65 vs 66) and no significant differences in co-morbidities. In this smaller and more closely-matched sample, those receiving the supplements still fared much better[4].
The second trial was conducted by Indian researchers and published in BMJ's Postgraduate Medical Journal. Consecutive patients admitted to a tertiary care hospital in north India with SARS-CoV-2 infection were randomized to either a vitamin D group or control arm. The enrolled patients were mildly symptomatic or asymptomatic with or without co-morbidities. At baseline, the subjects were similar in age and exhibited similar levels of inflammatory markers.
To be eligible for participation, all the patients had to exhibit vitamin D deficiency at baseline, defined as 25-hydroxyvitamin D levels below 20 nmol/L. The patients randomised to the supplement group received 60,000 IU daily of cholecalciferol a.k.a vitamin D3 (5 ml oral solution in nano-droplet form) for 7 days, with with the aim to achieve a 25 (OH)D level of >50 ng/ml. The control group was given a placebo (5 ml distilled water) for 7 days. All the participants received standard care for the SARS-CoV-2 infection and pre-existing co-morbidities as per hospital protocol.
Subsequently, 25(OH)D levels were assessed at day 7 and a weekly supplementation of 60,000IU provided to those with 25(OH)D >50 ng/ml or else continued on daily 60,000 IU supplementation until day 14 in subjects with levels under 50 ng/ml.
Forty participants were randomized (16 in the vitamin D arm and 24 to the control arm). Ten vitamin D participants achieved 25(OH)D levels of >50 ng/ml at day 7, and two more participants by day-14. Oral swabs were obtained for SARS-CoV-2 RNA detection at days 5, 7, 10, 14, 18 and 21 and detection was performed by real-time PCR testing.
Again, the vitamin D group fared significantly better. Ten of 16 (62.5%) participants in the vitamin D group achieved SARS-CoV-2 negativity compared to only 5 out of 24 (20.8%) participants in the control arm. The mean duration to SARS-CoV-2 negativity was 17.6 days.
Despite the very high vitamin D dose, no episodes of hypercalcaemia (excessive blood calcium) were observed[5].
More Trials to Come
While both trials were promising, and their results are in line with the research showing vitamin D protects against other ARIs, we need larger trials to make definitive public health recommendations about vitamin D and COVID-19. Also, while they indicate vitamin D could play an important role in COVID treatment, they they didn't examine its effect on preventing COVID infection.
I recently searched ClinicalTrials.gov, and found over 30 pending clinical trials involving vitamin D and COVID-19. Like the two trials we've just discussed, some will examine the vitamin's efficacy in treating existing COVID infection. Others will examine the vitamin's role in preventing COVID infection. A couple of Spanish trials and an Austrian study are specifically concerned with examining mortality outcomes. Some trials will utilize vitamin D solely, while others will employ vitamin D in combination with other nutrients and/or drugs (including HCQ).
Unfortunately, only three of these trials (from Brazil, France and Arizona) have been completed as of this writing, but they have no posted results as yet. Many are still recruiting participants and some are yet to even begin recruiting.
Sadly, research into vitamin D's effect on COVID does not enjoy the ability to travel at "warp speed," unlike the new and inadequately tested vaccines being rushed to market by the drug industry and our dystopian authorities.
In the meantime, there is no downside and much potential upside to supplementing with vitamin D. It's an essential vitamin of which many of us are deficient. The elderly, obese, dark-skinned people and people who wear long clothing year-round for religious or cultural reasons are even more likely to suffer vitamin D deficiency.
Vitamin D is relatively rare in our diet - our body relies primarily on sun exposure to form this vitamin. Of course, thanks to decades of anti-melanoma campaigns, many people have been conditioned to avoid even moderate sun exposure.
On top of all this, in order to 'prevent' COVID infections, our genius leaders have imposed lockdowns that force people to stay indoors, thereby ensuring an even greater prevalence of vitamin D deficiency. Which may increase the risk not only of respiratory tract infections, but other ailments like cancer, heart disease and osteoporosis.
It must also be noted that regular sun or artificial UV exposure does not make you immune from low vitamin D levels. In a study of 93 young adults living in Hawaii who reported being outside for an average of 22.4 hours weekly with no sunscreen, 51% had low vitamin D status of 30 ng/ml or less. The highest serum 25(OH)D concentration observed was 62 ng/ml[6].
An analysis of Boston subjects who used tanning beds found they had serum 25(OH)D concentrations almost double those of control subjects (115.5 vs 60.3 nmol/L, respectively). However, despite using a tanning bed at least once a week for 6 months or more, 8% of the tanners were vitamin D deficient (vitamin D deficiency among the non-tanners was 41.5%)[7].
Among 234 relatively healthy, ambulant and free-living elderly (60+) men living in tropical Brazil, the prevalence of vitamin D deficiency was 49.1% and 66.7% when cut-off points of less than 25 and 30 ng/mL, respectively, were used[8].
The only way to be certain of your vitamin D status is, of course, to get a blood test.
As Grant et al note in their review, the U.S. Institute of Medicine has acknowledged no adverse effects of vitamin D supplementation have been reported for daily doses under 10,000 IU/d.
For about half the population, write Grant et al, taking 5,000 IU daily of vitamin D3 or 30,000–35,000 IU weekly would raise 25(OH)D concentration to 40 ng/mL. Taking 6,235–7,248 IU/d would ensure 97.5% of the population has concentrations >20 ng/mL without exceeding the 10,000-IU/d threshold.
Magnesium supplementation is recommended when taking vitamin D supplements, note Grant et al. Magnesium helps activate vitamin D, which in turn helps regulate calcium and phosphate homeostasis to influence the growth and maintenance of bones. All the enzymes that metabolize vitamin D seem to require magnesium, which acts as a cofactor in the enzymatic reactions in the liver and kidneys. The magnesium dose should be in the range of 250–500 mg/d.
Certain drugs, such as Orlistat (Xenical) and corticosteroids impair vitamin D absorption from food and supplements, while cholestrol-lowering statins can impair vitamin D synthesis. My thoughts on statins are no secret: I think they are ineffective and toxic junk. As with antidepressants, they stand as a shining testament to the ability of Big Pharma to take useless and even counterproductive drugs and, by vigorous data diddling, buying off researchers and regulatory agencies, and clever marketing, transform them into multi-billion dollar blockbusters.
As for Orlistat, I can tell you from decades of researching fat loss and guiding people on diet/training programs that there are far better ways to get lean than taking a drug whose side effects include "oily spotting" of your underpants.
Thiazide diuretics decrease urinary calcium excretion; taking them with vitamin D supplements (which increase intestinal calcium absorption) might lead to hypercalcemia, especially among older adults and individuals with compromised renal function or hyperparathyroidism.
People with sarcoidosis, hypercalcaemia or high blood phosphate levels, kidney stones or kidney impairment should consult a competent medical practitioner before supplementing with vitamin D.
Conclusion
Vitamin D is cheap, effective against other types of acute respiratory tract infections, and is very safe, even at doses that would have conventional dietitians choking on their taste-free muffins. The same cannot be said for vaccines: While Big Pharma, governments, and the lamestream media have been doing all they can to portray the new COVID vaccines as safe as apple pie, the research indicates otherwise.
A FDA briefing document examining Pfizer-BioNTech's COVID-19 vaccine showed those who received the vaccine were far more likely to experience adverse events, including fatigue, headache, chills, muscle pain, joint pain and to require the use of pain medication (see below).
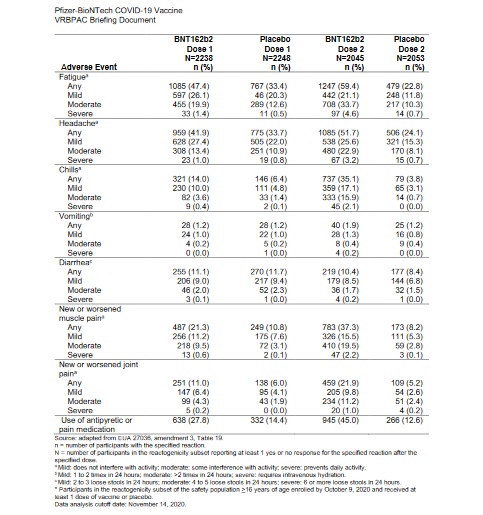 From p.36 of FDA Briefing DocumentPfizer-BioNTech COVID-19 Vaccine (https://www.fda.gov/media/144245/download).
From p.36 of FDA Briefing DocumentPfizer-BioNTech COVID-19 Vaccine (https://www.fda.gov/media/144245/download).
Wow. Take a drug with unknown long-term safety to avoid getting a largely asymptomatic flu virus, and instead get symptoms typical of a flu virus ...
I'll pass.
If You Found This Article Helpful, Please Consider Leaving a Tip
This site is self-funded and relies on reader generosity. Researching and writing articles like this takes a lot of time, so any and all tips are greatly appreciated!