
All around the world, people are being cajoled into taking the new and poorly tested COVID vaccines. The purpose of this coercion is supposedly to prevent a novel coronavirus whose fatality rate is measured in fractions of a percent.
In today's Reader Mail segment, we hear from someone being pressured to take the Pfizer-BioNTech COVID vaccine, and a reader who wants to know why the fatality rate figures I cite differ so much from the ones his friends uncritically recite.
"I'm Being Pressured to Take the Pfizer Vaccine"
"A" writes (emails edited and condensed for the sake of brevity):
Hi Anthony,
I’m getting pressure to take the Pfizer drug, so I thought I’d look up your stats. You said that there were 2,906 fatalities reported for [Tozinameran, the European brand name for Cominarty]. I went to the website you linked, manually selected each “Reaction Group” and added up the total “Fatal” figure for each one. Sure enough, they added up to exactly 2,906.
But, 3,000 fatalities out of 48 million injections isn’t really that bad, is it? Especially since they don’t necessarily know that the vaccine is what killed all of them. If I snapped my finger at 48 million people, some would probably die.
What am I missing?
A
My reply:
Hi A,
"But, 3,000 fatalities out of 48 million injections isn’t really that bad, is it?"
Compared to the figures for regular influenza vaccines, it's atrocious.
3,000 fatality reports for a drug that has yet to demonstrate it can save a single life is appalling.
And remember, your postulation does not accommodate the fact that the vaccine adverse event report figures are underestimates, while the COVID death figures are wild exaggerations.
It is well-known these databases capture only a small portion of the total adverse event cases. Even the CDC estimated only 13% of reactions to influenza vaccines are reported to VAERS.
And the story doesn't end with deaths; go back and check out the figures for non-resolved issues. Visit the VAERS database and check out the figures for permanent disability, hospitalization, etc.
What doesn't kill you may leave you in a bad way, sometimes permanently.
These are poorly studied drugs and, all mainstream propaganda to the contrary, we simply do not know their long-term effects. The longest follow-up data published so far for any of these pseudo-vaccines after second injection is a big fat four months (that's the South African data for the Oxford-AstraZeneca drug, which failed to show efficacy for even mild-moderate infection of the dominant COVID strain there).
Which brings us to the highly inconvenient issue of efficacy. Even if only 1 life is taken from these new vaccines, that is 1 life more than they have been shown to save under alleged double-blind conditions.
The Pfizer-BioNTech drug has triggered 2,906 fatality reports in Europe alone but is yet to demonstrate it can save even a single life. We do however know it causes a vast array of side effects - that much the research does show.
Which means at this point the drugs possess a wholly unacceptable risk: reward ratio.
There's also the question of whether you will allow a confirmed criminal enterprise like Pfizer, whose past misdeeds include manipulating research data, to start tinkering with your messenger RNA and insert artificial instructions into your cells.
Modesty forbids me from reprinting the exact language I would employ if personally asked to do this.
In fact, I find that proposition so ridiculous that, in normal times, I would have to wonder if it was a trick question.
In regards to your comment, "Especially since they don’t necessarily know that the vaccine is what killed all of them. If I snapped my finger at 48 million people, some would probably die."
Would you mind relaying this to all the dishonest authorities around the world who labelled deaths that had nothing to do with COVID-19 as COVID-19 fatalities? In the US, the situation was so ridiculous that even a murder-suicide case was listed as two COVID-19 deaths because the perpetrator and victim allegedly tested positive for the virus within 30 days of their violent deaths.
Anthony Fauci and Deborah Birx even admitted at a 7 April 2020 White House press conference that deaths from causes such as heart disease and kidney failure were being listed as COVID-19 deaths - and no-one batted an eyelid.
 Anthony Fauci and Deborah Birx.
Anthony Fauci and Deborah Birx.
But in response to a continuing stream of reports about otherwise healthy people falling violently ill and dying soon after getting these poorly tested Brave New World COVID drugs, the same authorities are bending over backwards to absolve the vaccine of any causal role.
I guess what you need to decide is if you are prepared to be injected with a drug made by a criminal enterprise, using poorly studied and problematic mRNA technology that, prior to this COVID farce, had never even made it to Phase 3 testing let alone been approved for human use. A drug that also contains PEG, which has no place inside your cells, a drug which has racked up an alarming number of adverse event and death reports in a short time.
For me, that's a not a hard question.
Before I close off, I note that in your original email you said you were being pressured into taking the vaccine. That right there should tell you a lot. I'm not sure where you are writing from, but you may want to check what legal protections are afforded to you in your jurisdiction against parties who are trying to coerce you into undergoing poorly studied and problematic medical therapies that are still in the experimental phase of research. Repeated claims that these vaccines have been been Thoroughly Tested!™ and proven Safe and Effective!™ are demonstrably false.
We are in the unprecedented situation in which these drugs were released to market despite not having gone through the proper new drug approval processes. All for a non-pandemic whose severity pales in comparison to past genuine pandemics such as the Spanish Flu. Despite occurring over a hundred years ago among a far smaller global population, the Spanish Flu of 1918 killed an estimated 50 million people.
As of this writing, even the wildly inflated COVID-19 death toll amounts to a far lower figure of just under 2.8 million deaths worldwide.
Here in Australia, the Federal Health Minister Greg Hunt admitted, when discussing the unknown longevity of the antibody response of these new vaccines, "the world doesn't know that answer, the world is engaged in the largest clinical trial, the largest global vaccination trial ever." (See 12:40 onwards in video below). Hunt was later rushed off to hospital only two days after getting the AstraZeneca vaccine, suffering a severe case of cellulitis.
Either he didn't get the memo that this is all a complete sham or, like a lot of Australians, he foolishly believed he could put a dodgey drug into his body without consequence (Australians share global top spot along with New Zealanders and North Americans for per capita illicit drug use).
Everyone who takes this vaccine is participating in an ongoing experiment, the ultimate outcome of which is unknown. You may wish to read what the Nuremberg Code has to say about "Permissible Medical Experiments."
Best of luck whatever you decide,
Anthony.
"A" replies:
Hi Anthony,
wow, that’s a lot to take in. I’d like to understand more about your statement that the vaccines have yet to demonstrate that they can save a single life. How would one measure that?
If a person tests positive for antibodies, then you could argue that whatever the risk is for a person with their health profile and age, that person will avoid that risk for having taken the vaccine, no? I don’t understand how this is measured.
A.
My reply:
Hi A,
Re: "I’d like to understand more about your statement that the vaccines have yet to demonstrate that they can save a single life. How would one measure that?"
Easy. You get independent, impartial entities to conduct placebo-controlled, double-blind clinical trials of the vaccines.
You would do this to eliminate the numerous confounders inherent in other forms of 'evidence.' For example, claims that the vaccines are reducing the real world COVID-19 infection and death rates are disingenuous given all the other factors that are concomitantly playing out.
For starters, you have the well-documented development of natural immunity that occurs in response to new infectious pathogens. So we would fully expect to see COVID-19 cases and fatalities decline and eventually peter out to low levels - as has happened with pretty much every other flu outbreak in history.
You also have the well-established dishonesty and chicanery of governments and health authorities. It is interesting that, in the US, the COVID death figures began declining in tandem with Trump's chances of retaining his presidency. And on 20 January 2021 - the very same day the establishment's preferred puppet, Joe Biden, was officially installed as POTUS - the China-controlled World Health Organization issued much stricter guidelines for PCR testing of COVID-19. Which of course will dramatically lower the astronomical number of false positives these tests are known to trigger.
It doesn't get much more blatant than that.
C'mon man!
Speaking of remarkable coincidences, feast your eyes upon this graph from the EUROMOMO website:
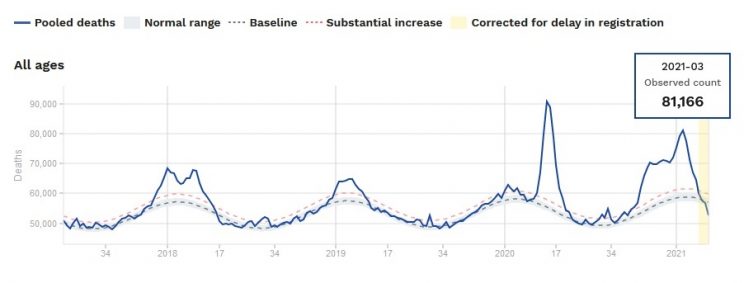 Source: https://www.euromomo.eu/graphs-and-maps (captured 29 March 2021).
Source: https://www.euromomo.eu/graphs-and-maps (captured 29 March 2021).
As you can see, overall "second wave" mortality for the 26 included European countries peaked in the third week of January - the same week WHO tightened up its testing criteria. After that, the death rate dramatically plummeted.
The sudden drop is seen in all ages from 15 up.
And this in the middle of the European winter, mind you, a time when sunlight exposure and vitamin D status, and hence natural immunity, would be at annual lows.
These figures, it must also be noted, are for overall mortality, not just COVID deaths. And they beggar belief. Never before have I heard of people from different countries coming together to postpone their deaths because the United States had just installed a senile, hair-sniffing, little girl-grabbing, money-laundering creep as its new president!
It is truly unprecedented. Then again, there are a lot of things about this COVID charade that are truly unprecedented.
I find this highly suspicious and indicative of data tampering (you wouldn't need to modify the data for every country, just the ones whose mortality rate remained high at the time of the new WHO testing mandate).
But even if we take the remarkable trajectory in the above graph at face value, it still fails to affirm a beneficial role for vaccines.
Which is exactly what vaccine shills are already claiming: That their beloved drugs are responsible for the decline in deaths.
Problem is, they have no proof of this. If you scroll down the page where the above graph was sourced, you'll note that the decline of the so-called 'second wave' began in numerous countries well before the vaccine rollout. For some readily identifiable examples, check the graphs for Greece, Hungary, Italy, Slovenia, Austria and Belgium.
This is why we have double-blind, placebo-controlled trials - to bypass the numerous confounders and discrepancies inherent in epidemiological evidence. In these trials, people are randomly assigned to either a drug or placebo group. Neither the participants nor researchers know who is getting what, until after the study is over and the results have been tabulated and analyzed.
To prevent bias and data manipulation, these trials should be conducted by independent entities with no vested financial interests in the results. Research has repeatedly shown that studies conducted or sponsored by vested interests are far more likely to return positive results for those interests' products.
Sadly, none of this has yet happened with the COVID vaccines.
All the trials have been sponsored and conducted by the manufacturers. Two of these, AstraZeneca and Pfizer, have long histories of criminal convictions and settlements for dishonesty offences. Moderna, meanwhile, is an aggressively entrepreneurial company that former insiders describe as being far more concerned with its share price than sound science.
The majority of the AstraZeneca trial arms published thus far have been single-blind only, meaning the researchers knew who was getting the vaccine and who wasn't.
Which is, quite frankly, a farce.
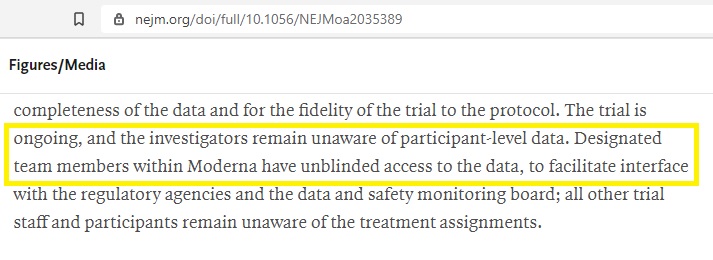
The Moderna trial is supposedly double-blind, but it really isn't: Numerous Moderna employees in fact have unblinded access to the ongoing trial data!
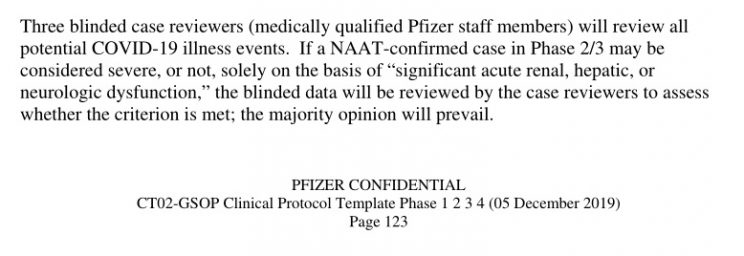
In the single Pfizer trial that has been thus far reported, three Pfizer employees were in charge of reviewing all COVID-related events! Even if they remain blind to the origin of these events, it wouldn't be hard to guess given that four times as many participants in the drug group have required pain and anti-inflammatory medications to combat the vaccine's side effects.
Also, the Pfizer study contains a highly suspicious and unexplained discrepancy, in which hundreds of extra vaccine participants were mysteriously excluded from the study for no given reason. Given Pfizer's established history of manipulating data and suppressing unfavourable research results, this raises the possibility that COVID cases and deaths in the drug group were conveniently excluded from the study using this vague, catch-all category.
And the real cracker is that, even with all these advantages, the trial data has failed to demonstrate that any of these 'vaccines' can save even a single life.
How do I measure that? Simple. By looking at the death data in all of the papers that have been published so far.
All show low death rates. In the allegedly double-blind trials, none of these are confirmed COVID deaths, irrespective of whether they occurred in the treatment or placebo groups. The only data claiming a single COVID death in the placebo group was from an AstraZeneca trial arm - but that arm of course was non-blinded to the researchers and the control treatment was in fact a meningococcal vaccine, not a saline placebo!
In the one AstraZeneca trial arm published so far that was reportedly double-blind (in South Africa), the drug failed to show efficacy against even mild-moderate infection with the dominant strain of COVID there. There were no deaths or hospitalizations in that study.
"If a person tests positive for antibodies, then you could argue that whatever the risk is for a person with their health profile and age, that person will avoid that risk for having taken the vaccine, no? I don’t understand how this is measured."
You can argue all sorts of things. I can argue there are invisible leprechauns under my desk who dance the tarantella (they're Irish-Italian leprechauns, you see). Even if I really believed this highly unlikely proposition, the onus would still be on me to provide proof to others.
Using seemingly logical rationalizations ("oh, the reason you can't see the invisible leprechauns is because they're invisible" or "vaccines create antibodies, antibodies protect against infection, COVID vaccines create antibodies, therefore the COVID vaccines prevent COVID infection and deaths!") is not proof.
It's not even evidence.
It's just unsubstantiated conjecture.
Again, I refer you back to the clinical trials, which I have dissected and discussed in detail in the following articles:
Pfizer-BioNTech vaccine:
Pfizer-BioNTech COVID-19 Vaccine: The ‘Life-Saving’ Drug that Seems to be Killing People
Oxford-AstraZeneca vaccine:
The Appalling Science and Conflicts of Interest Behind the Oxford-AstraZeneca COVID-19 Vaccine
Latest Clinical Trial Data Shows AstraZeneca COVID-19 Vaccine is Useless
Moderna mRNA vaccine:
The Junk Science Behind the Moderna COVID-19 Vaccine
This isn't rocket science. If you are going to claim a drug saves lives, you can't just pull that claim from your nethermost regions and get your billionaire media-owning buddies to repeat it ad nauseum until people believe it.
Actually, you can, and that's exactly what is transpiring. But repeating a falsehood over and over until most people simply assume its true is not the same thing as scientific proof.
To honestly claim a drug has been proven to save lives, you need to first demonstrate that contention under non-biased, double-blind, placebo-controlled conditions. That hasn't even come close to happening with any of the COVID-19 vaccines.
If you are after a simple, non-toxic method of protection from COVID-19 and other pathogens, one that does not involve supporting criminal enterprises and getting injected with dubious and poorly tested drugs, check out the research for vitamin D. I simply don't have the time to go into it now, but do intend to address the topic when time permits. In the meantime, this website will get you started.
Kind regards,
Anthony.
What's the Real Fatality Rate of COVID-19?
"D" writes:
Dear Anthony,
You keep mentioning a COVID-19 death rate of <0.5%, which I quote to friends who fully accept all the government propaganda and lies.
They then come back with X cases / Y deaths is not <0.5%, but more like 2.5%.
Please give me your reasoning so I can refute.
Many thanks,
D
My reply:
Hi D,
people are confusing - by accident or design - infection fatality rate (IFR) and case fatality rate (CFR).
Case fatality rate does not tell you how many people who become infected with a virus will die. It only tells you how many of those who present to a medical facility for treatment are likely to die. When they seek treatment, they become "cases."
The big problem with CFR is that only a tiny portion of people who get an influenza infection will ever show up to a hospital. Think of all the times in your life you got the flu - how many of those times did you rush into an emergency ward yelling "help, my nose is runny and I've got a bad cough!"
CFR represents the more serious infections, the ones that require medical assistance. Because the overwhelming majority of influenza cases do not require medical assistance, CFR is hopelessly skewed and does not even begin to represent the true overall fatality rate of a virus.
Infection fatality rate is what really counts. And the way you get an idea of IFR is to randomly test large samples of the population for the target virus, whether they are symptomatic or not. You then compare the number of people who tested positive with the number of people among that population who have died from the virus in a given and recent time frame.
When you do that, the 'deadly' coronavirus suddenly isn't so deadly.
I have linked to a number of such analyses in previous articles, but there is a new one hot off the press that I'll discuss in a moment. Before I do so, I'll reiterate even the CDC has long posted 'best guess' COVID-19 IFR estimates that belie the hysteria.
COVID-19 IFR estimates have declined over time, something one would expect in the face of increased testing and naturally-acquired herd immunity. It is most curious then that, as controversy over the COVID vaccines mounts, the dishonest CDC has recently increased its IFR estimates. For each age group, the CDC's current COVID-19 IFR rates are:
0-17: 0.002% (similar to previous 0.003%)
18-49: 0.05% (increased from 0.02%)
50–64: 0.6% (increased from 0.5%)
65+: 9.0% (increased from 5.4%)
Even after their recent and suspicious inflation, the CDC figures still evince a very low IFR - under 1% in every age group except over 65s.
Now, to the new IFR analysis by Dr. John Ioannidis that has been posted online in the European Journal of Investigation.
Unlike the hopelessly biased and dishonest CDC, Dr. Ioannidis (Professor of Medicine, Health Research and Policy, and of Biomedical Data Science at Stanford University School of Medicine) is a highly respected researcher who is not afraid to tear strips off the mainstream's most sacred cows. His 2005 paper "Why Most Published Research Findings Are False" is the most-viewed article in the history of the Public Library of Science, with more than 2.6 million views (the next most widely-viewed, believe it or not, is a paper by Prause et al titled "Women's Preferences for Penis Size: A New Research Method Using Selection among 3D Models").
On 17 March 2020, Ioannidis authored a STAT op-ed critical of the world's COVID response. If you take the time to read it, you'll see it was quite sensible and cautious in its tone. Upholders of the mainstream COVID-19 narrative, however, promptly blew their gaskets. But Ioannidis was eventually proven correct: The world rushed to impose draconian restrictions that were not based on sound data.
There is abundant research to show lockdowns don't work and cause more harm than good, and that mask mandates are ineffective. Countries that did not institute lockdowns are doing just fine. Sweden, which shunned lockdowns, has a lower per capita rate of COVID deaths than Portugal, despite their similar population sizes.
Ioannidis' new paper can be accessed in full here. Based on his analysis, the best estimate global IFR average for COVID-19 is around 0.15%.
In Europe and the Americas, the likely IFR is around 0.3-0.4%. When institutionalized people are omitted and the analysis confined to community-dwelling folks, the IFR estimate for those regions was ~0.2%.
As I explained to "A" above, this is not the Spanish Flu.
It's all well and good for the media to present heartbreaking stories of people who were allegedly "struck down" by COVID-19. Using stories with emotional impact is always a great way to bypass people's rational faculties, and the media knows it.
Abandoning the usual discreet and respectful manner of transporting the recently deceased, and instead piling up their corpses in churches, as authorities did in Italy, or making a point of loading their dead bodies into trucks out in the street in broad daylight (as occurred in Communist Cuomo New York), makes for great sensationalist headlines. But people should see it for what it is: Disgraceful, government-orchestrated street theatre designed to give the impression there is a monster virus on the loose and that we should all cower in fear and do everything our corrupt, lying and hopelessly hypocritical authorities tell us.
But when you look at the science, there is just nothing to support the COVID-19 hysteria. It might have been cooked up in a Wuhan lab with nefarious intentions, but it's nevertheless a mild virus with a very low fatality rate.
Cheers,
Anthony.
If You Found This Article Helpful, Please Consider Leaving a Tip
This site is self-funded and relies on reader generosity. Researching and writing articles like this takes a lot of time, so any and all tips are greatly appreciated!