
The lunacy continues.
The world is still soiling its pants over a relatively harmless flu virus.
Amidst constant rumblings about a “second wave,” many countries around the world are still in various states of lockdown, and many still have travel bans in place.
The wholly unwarranted COVID-19 hysteria has been used to impose unprecedented human rights restrictions upon much of the world’s population – including draconian restrictions on freedom of movement, removal of the right to assembly, even the right to gather with one’s friends and family for culturally important events such as weddings and funerals.
Homo sapiens are inherently social and interactive creatures, but are now being forced and fined into an utterly unnatural and inhuman state of isolation, as “social distancing” becomes the “new normal.”
The indisputable fact is that gathering with friends and family, and interacting peacefully with fellow citizens, is a perfectly normal, healthy and essential activity, but people in many countries are now being harshly scolded and fined for doing so.
According to the World Health Organization, every country had some form of travel ban by 20 April 2020 – the most extensive travel restriction campaign in history. This is despite a paucity of evidence that travel bans slow infection in countries where outbreaks have already kicked off, and an abundance of evidence showing the bans are destroying the travel industry, with a forecast loss of 100 million jobs.
Coupled with the destruction of business – especially small business - and the hundreds of millions of job losses around the world, this utterly insane state of affairs is leading to a global increase in depression, anxiety and suicide rates.
People have become so paranoid of catching the largely harmless COVID-19 influenza they are even staying away in droves from emergency wards despite suffering truly deadly health ailments. Deaths at home are increasing as impressionable patients shy away from intensive care units.
You’ve Been Massively Conned, Folks
What I am about to say will no doubt offend many of the people who have been blinded by the Great COVID-19 Con, but I make absolutely no apologies for pointing out what should be obvious to anyone with even half a brain:
The alarmism surrounding COVID-19 is complete and utter bullshit.
This alarmism has nothing to do with the actual health risk posed by the virus itself.
Despite all evidence pointing to a laboratory origin, COVID-19 is like most seasonal flu strains in that it has a low mortality rate and poses no mortality risk to over 99% of people who become infected.
If you earnestly believe an unprecedented abrogation of fundamental human rights, the imposition of an anti-social “new normal,” increased misery and suicide worldwide, global economic devastation, international travel bans and an alarming increase in police state behaviour is justified by a flu virus with an infection fatality rate of less than 1% then …
… you are a fucking idiot.
Do you really believe that every time a novel flu outbreak occurs, the world must go into a state of collective house arrest?
What happened to letting our immune systems do what they’ve evolved over millions of years to do? What happened to the exalted “herd immunity” concept that vaccine shills incessantly bang on about? Or is herd immunity only desirable when it comes from highly profitable vaccine vials?
If you really think this whole paranoia campaign is about health, you are terribly misguided.
If you think it is just pure coincidence that, as millions of people around the world lost their jobs, the world’s billionaires became even wealthier during the lockdown, then you are part of what is wrong with the world. Your hopeless gullibility is why the world’s ultra-rich are able to enact their malfeasant, self-serving agendas with so little resistance.
Harsh words?
Considering the global devastation being caused by this COVID-19 scam, and what lies in store for humankind, I think I’m actually being quite polite.
I will now explain just why the paranoia surrounding COVID-19 is completely unfounded nonsense.
The ‘Deadly’ Coronavirus Is Not Very Deadly At All
When I wrote about COVID-19’s likely laboratory origins back in May, the US Centers for Disease Control and Prevention (CDC) had issued a “best estimate” infection fatality rate for COVID-19 of 0.4%. This meant that, of all people infected with the virus, the most likely scenario was that less than one-half of one percent would die.
Since I penned that article, the world seems to have strangely lost interest in how the virus really originated. The ever-influential mainstream media is diverting attention away from this prickly issue, instead reinforcing the “deadly virus” narrative and perpetuating “second wave” fears.
The mainstream media is also obsessed with the “race” for a vaccine. Of all the possible strategies humankind could have embraced in battling this novel virus, the mainstream media has played a key role in placing lockdowns, social distancing and a vaccine at the forefront of public consciousness.
The remarkable success of this propaganda campaign can be gleaned by the fact that most people - laypersons and trained medical professionals alike - earnestly seem to believe these are the only viable strategies for combatting the virus.
In step with this doubling down of ‘”deadly virus” rhetoric, the CDC has slightly revised its most recent ‘best estimate’ COVID-19 infection fatality rate upward from 0.4% to 0.65%. The CDC also presents a best guess estimate that 40% of those infected will show no symptoms.
How accurate are these estimates?
According to multiple studies where researchers actually bothered to do widespread testing, they are both wrong.
One of the problems in ascertaining mortality estimates for a relatively mild flu virus is we don’t know how many people are infected. The CDC even admits it cannot estimate with any certainty what percentage of people who catch regular influenza each year will die, because it is impossible for them to know just how many people actually catch the flu. Many people show little to no symptomology, and hence will never be recorded on official records. Even people who get discernibly sick and succumb to a bad case of flu will often ride it out and wait for nature to take its course, instead of running to the doctor or nearest hospital.
So even if you have an accurate count of people who died from an often asymptomatic infection like COVID-19, it remains difficult to calculate overall mortality rates when you don’t know how many people were infected overall.
As Eran Bendavid from Stanford University School of Medicine, and his colleagues, point out, "many epidemic projections and policies addressing COVID-19 have been designed without seroprevalence data to inform epidemic parameters."
In other words, our officials and ‘experts’ have been wanking on about the virulence of COVID-19 and formulating draconian policies without considering data on how prevalent the virus really is.
That’s like a mechanic ordering a part for your car when he doesn’t even know what car you drive.
Kinda moronic.
And so on 3 and 4 April 2020, Bendavid and his colleagues tested a random sample of Santa Clara County, California residents for antibodies to SARS-CoV-2. The sample included 3,330 adults and children recruited via Facebook ads.
At the time of the study, Santa Clara County had approximately 1,000 confirmed SARS-CoV-2 cases, the largest number of any county in Northern California. The county also had several of the earliest known cases of COVID-19 in the state - including one of the first presumed cases of community-acquired disease - making it an especially appropriate location to test a population-level sample for the presence of active and past infections.
After adjusting for county demographics and test specificity and sensitivity, the best estimate for the prevalence of antibodies to SARS-CoV-2 in Santa Clara County in early April was 2.8%, with a possible range of 1.3% to 4.7%.
This implies that, by 1 April 2020 around 54,000 people had been infected with COVID-19 in Santa Clara County.
Compare this with the reported number of confirmed positive cases in the county on 1 April 2020, which was a mere 956 – that’s 55-fold lower than the number of infections predicted by this study. Even using the lowest estimate from the possible range indicates a 26-fold higher prevalence, while the highest possible figure of 4.7% would mean a 95-fold underestimation of actual cases!
Through 22 April 2020, 94 people were officially ascribed as dying from COVID-19 in the County. Assuming a 3 week lag from time of infection to death, then 94 deaths out of 54,000 infections corresponds to an infection fatality rate of 0.17% in Santa Clara County.
The Bendavid study drew criticism from some researchers, who claimed the method of recruitment (Facebook) may have drawn people with symptoms who wanted free testing, hence overestimating the prevalence. The opposite, however, could also be true. Participants in health studies tend to have an interest in health, and as a result often practice healthier lifestyle habits (a phenomenon dubbed the Healthy User Bias).
The Santa Clara survey may have been further skewed to healthy participants because it selected for members of the population who were able to drive to the testing site. Not only could this have excluded some people feeling 'under the weather,' it would have skewed the sample away from certain high risk groups such as homeless populations and nursing home residents.
Furthermore, the Bendavid et al estimates are in line with those obtained further south in the Golden State, and downright modest when compared to those in some other states and countries.
Testing conducted in Los Angeles County on 10 April 2020 estimated a SARS-CoV-2 seroprevalence of 4.1%. Adjusting this estimate for statistical margin of error indicated 2.8% to 5.6% of the county's adult population had antibodies to the virus - which translated to approximately 221,000 to 442,000 adults in the county having had the infection. That estimate is 28 to 55 times higher than the 7,994 confirmed cases of COVID-19 reported to the county by the time of the study in early April. By 20 April, the number of COVID-related deaths in the county had surpassed 600, implying an infection fatality rate of only 0.14% - 0.27%.
Testing in New York, a city providing a constant source of alarmist fodder for the mainstream media, also indicates official infection rates are grossly understated. Researchers from the New York-Presbyterian/Columbia University Irving Medical Center gave COVID-19 tests to pregnant women presenting to deliver babies between March 22 and April 4. Of 215 women, four had symptoms. All four tested positive. Swabs were also obtained from 210 of the 211 asymptomatic women, with 29 testing positive. Of those 29 asymptomatic women, four later developed symptoms, but 25 never did.
Overall, 15.4% of the women tested positive for COVID-19, and 87.9% of those testing positive showed no symptoms upon presenting to the hospital.
Random testing of 3,000 supermarket customers across New York State in mid-April returned a positive rate of 14 percent, according to the state's Governer, Andrew Cuomo. This suggested the true incidence of the virus amounted to more than 1.7 million people in New York City, and over 2.6 million people state-wide - far greater than the 250,000 officially recorded cases. It would also mean the fatality rate from the virus was relatively low, about 0.5 percent, Cuomo acknowledged.
Testing at Massachusetts homeless shelters has found even higher rates of infection. Forty-three percent of the population at a Worcester adult emergency homeless shelter tested positive for COVD-19 in April. Most of those testing positive were asymptomatic or "very minimally symptomatic," according to one of the researchers, Dr Erik Garcia.
At Boston's Pine Street Inn shelter, 397 people were tested, with 146 (36%) coming up positive. Every one of these folks was asymptomatic. None had a fever, and none of them reported symptoms.
Keep in mind your average homeless person is unlikely to be enjoying optimal nutrition and hygienic living arrangements, yet the immune systems of most of those tested were clearly having little difficulty dealing with the virus.
Studies conducted overseas also indicate a higher infection rate and much lower mortality rate than previously claimed.
Iceland’s Experience
Iceland did not impose a full national lockdown, and most shops and businesses remained open. Its restrictions are largely based on trust, although the country did ban gatherings of more than 20 people. Like other localities such as Taiwan, Singapore and Hong Kong that have moderately-sized populations and relatively diminutive geographies, Iceland has proved successful at "flattening the curve."
By 11 April 2020, Iceland had achieved something no other country had: It tested 10% of its population for COVID-19, a figure far higher than anywhere else in the world. Of Iceland's 1,600-plus infections as of 11 April, seven ended in deaths, indicating a fatality rate of around 0.4%.
Keep in mind Iceland is one of the world’s northernmost countries, and was coming out of the Northern Hemisphere winter, so was likely at a distinct disadvantage in terms of sunlight exposure and vitamin D status. Yet the country’s COVID-19 fatality rate was only 0.4%.
In early April, the entire population of the town of Robbio, Italy, was invited to undergo COVID-19 testing. A third of the town’s 6,000 residents were tested in 48 hours, with 13-14% of the analysed sample showing antibodies to COVID-19. Media reports on the official infection rate at the time vary slightly, with a 2 April 2020 story citing 27 officially-recognized positive residents and 4 deaths. On 9 April 2020, Business Insider Italia cited an official figure of 23 positive patients in Robbio. Either way, widespread testing again showed the official infection rates to be hugely understated.
In the rural town of Gangelt, dubbed Germany’s 'Wuhan' because it was the site of the country's first COVID-19 fatalities, 500 of the town's 12,000 inhabitants were tested. The results indicated 15 per cent of the population was believed to have been infected, compared to the official 1% figure for the Heinsberg region in which Gangelt is situated. This figure suggested a COVID-19 mortality rate in the town of 0.37 per cent - less than one-fifth of the officially-recognised mortality rate in Germany at the time.
All these studies were conducted and publicized in early-to-mid April, meaning officials and ‘experts’ around the world have had almost four months to digest their results. But instead of acknowledging they have been grossly exaggerating the lethality of COVID-19, they continue to bombard us with a relentless storm of alarmist bullshit in order to justify their continued draconian police state behaviour. The CDC has even revised its best guess fatality estimate upwards!
I will reiterate: If you earnestly believe a virus whose fatality can be measured in fractions of a percent justifies a global lockdown that is destroying innocent people’s livelihoods and driving them to suicide, and crushing the civil liberties of those who remain, then you are an irredeemable moron.
Exaggerating the COVID-19 Death Data
In countries such as the US and UK, the official fatality rate may be even lower than these studies indicate, because there is ample evidence to show authorities have been systematically inflating the death statistics for COVID-19.
A key factor enabling such exaggeration is the issuance of guidelines making it remarkably easy to ascribe COVID-19 as the cause of death, even in cases where there is little-to-no proof.
Under normal circumstances, cause of death is attributed to - surprise, surprise - the underlying cause. In other words, if a patient with coronary heart disease becomes infected with "regular" influenza and suffers a fatal myocardial infarction (heart attack), the cause of death would normally be listed as myocardial infarction, not influenza. Influenza may have weakened the patient and hastened the onset of a heart attack, but it was still a heart attack that killed him – not a bad cough or sore throat. Researchers have known for years heart attack fatalities rise during influenza season (I wrote about this in my 2006 book, The Great Cholesterol Con), but no matter - those deaths are largely ascribed to heart attack, not influenza.
And in its recent recommendations to physicians when writing up death certificates, the UK's Office for National Statistics even admits - in a single line buried on page 5 of the 17-page document - that "Most routine mortality statistics are based on the underlying cause."
However, when it comes to COVID-19, long-established guidelines for ascribing cause of death have suddenly been tossed out the window. In its guidelines for completing the medical certificate cause of death (MCCD), the ONS announces:
“In an emergency period of the COVID-19 pandemic there is a relaxation of previous legislation concerning completion of the medical certificate cause of death” [Bold emphasis added]
It continues:
"Without diagnostic proof, if appropriate and to avoid delay, medical practitioners can circle ‘2’ in the MCCD (“information from post-mortem may be available later”) or tick Box B on the reverse of the MCCD for ante-mortem investigations. For example, if before death the patient had symptoms typical of COVID-19 infection, but the test result has not been received, it would be satisfactory to give ‘COVID-19’ as the cause of death, tick Box B and then share the test result when it becomes available. In the circumstances of there being no swab, it is satisfactory to apply clinical judgement."[Bold emphasis added]
This advice is extraordinary - in all the wrong ways.
If a patient has symptoms "typical" of COVID-19, the ONS considers it perfectly acceptable for doctors to rush ahead and list COVID-19 as the official cause of death - even when no test results are available to confirm this!
It bears reminding that testing for COVID-19 is about as easy a diagnostic procedure as you’ll get; the physician doesn’t even need to draw blood. Rather, a Q-tip is inserted into the patient’s nasal cavity or throat, and then the resultant swab is handed to the pathology lab for testing.
Perhaps the failure to perform this simple test would not be so egregious if COVID-19 presented with its own very unique set of symptoms. But the "typical" symptoms of COVID-19 are very similar to those of regular influenza. Don't take my word for it - here's the CDC's own description:
"People with these symptoms may have COVID-19:
Cough
Shortness of breath or difficulty breathing
Fever
Chills
Muscle pain
Sore throat
New loss of taste or smell
This list is not all possible symptoms. Other less common symptoms have been reported, including gastrointestinal symptoms like nausea, vomiting, or diarrhea."
Incredible. Each and every one of those symptoms is common to your "garden-variety" influenza that strikes every winter, every year. Those symptoms also overlap with a myriad of other common health conditions.
But in a world that has been scared senseless into believing it is about to be wiped out by a super-deadly COVID-19 pandemic, it's not hard to see how doctors would be subconsciously swayed into designating COVID-19, instead of influenza or other conditions, when they "apply clinical judgement."
The World Health Organization has fully enabled this charade by introducing two new International Classification of Diseases (ICD) codes for COVID-19: "U07.1 COVID-19, virus identified" and "U07.2 COVID-19, virus not identified" which is so-called "Clinically-epidemiologically diagnosed COVID-19" that includes "Probable COVID-19" and "Suspected COVID-19."[Bold emphasis added]

Over in the US, increasing evidence is emerging that other not-so-subtle forces are being brought to bear upon doctors' "clinical judgement" when determining COVID-19's role in patient deaths.
COVID-19: The Disease for Which Assumption Overrides Confirmation
In an alert dated 24 March 2020, Steven Schwartz, Director of the Division of Vital Statistics at the CDC's National Center for Health Statistics, gave the following advice to doctors in Q&A style:
"What happens if the terms reported on the death certificate indicate uncertainty?
If the death certificate reports terms such as “probable COVID-19” or “likely COVID-19,” these terms would be assigned the new ICD code. It is not likely that NCHS will follow up on these cases. [Bold emphasis added]
Should 'COVID-19' be reported on the death certificate only with a confirmed test?
COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death." [Bold emphasis added]
As in the UK, uncertainty and a lack of pathology results are no impediment to officially "assuming" a “probable COVID-19” or “likely COVID-19” death - even though testing for active COVID-19 is no more invasive than taking a nasal or throat swab.
Schwartz's easy-going approach to ascribing COVID-19 as a cause of death was reflected in another CDC advisory, issued in April, which told physicians:
"In cases where a definite diagnosis of COVID–19 cannot be made, but it is suspected or likely (e.g., the circumstances are compelling within a reasonable degree of certainty), it is acceptable to report COVID–19 on a death certificate as “probable” or “presumed.” In these instances, certifiers should use their best clinical judgement in determining if a COVID–19 infection was likely. However, please note that testing for COVID–19 should be conducted whenever possible."[Bold emphasis added]
What doctors are basically being told is, “it would be nice if you did actual testing but, hey, if you don’t – no stress. We’re happy to accept ‘probable’ and ‘assumed’ COVID-19, even though the diagnostic procedure is no more complicated than taking a quick swab. Don’t even begin to worry about repercussions for ascribing the wrong cause of death, because we’re not going to double-check any deaths ascribed to COVID-19.”
During an April 9 interview on Fox News, Scott Jensen, a Minnesota family doctor and Republican state legislator, called the CDC's advice "ridiculous" and contrary to usual medical practice. "The idea that we're going to allow people to massage and sort of game the numbers is a real issue, because we're going to undermine the [public] trust," he said.
Cash for COVID-19
Dr Jensen also noted hospitals have a financial incentive to over-diagnose COVID-19. "Any time health care intersects with dollars, it gets awkward," he said. "Right now Medicare has determined that if you have a COVID-19 admission to the hospital, you'll get paid $13,000. If that COVID-19 patient goes on a ventilator, you get $39,000—three times as much. Nobody can tell me, after 35 years in the world of medicine, that sometimes those kinds of things [don't] impact on what we do."
Jensen clarified in the video that he doesn't think physicians are "gaming the system" so much as other "players," such as hospital administrators, who he said may pressure physicians to cite all diagnoses, including "probable" COVID-19, on discharge papers or death certificates to get the 20% higher Medicare allocation allowed under the Coronavirus Aid, Relief and Economic Security Act.
Hospitals are effectively being bribed into assigning COVID-19 as the cause of death wherever possible.
Health Department Falsely Altered Death Certificates
On 14 May 2020, a Republican state representative asked prosecutors to bring criminal charges against Colorado’s top public health official, claiming that she illegally falsified death records to inflate COVID-19 death totals. Rep. Mark Baisley (R-Roxborough Park) accused Jill Ryan, executive director of the Colorado Department of Public Health and Environment (CDPHE), of “falsely altering death certificates.” CDPHE collects and reports COVID-19 statistics from across Colorado.
Baisley provided another letter dated 17 April 2020 from the Someren Glen senior care center to its staff, residents, and residents’ families. The Centennial facility's letter said CPDHE had overruled the cause of death findings by attending physicians in order to list seven deaths as being caused by COVID-19.
“We have never seen a situation where the health department overrules a physician’s findings,” the letter provided by Baisley reads. “However, these are unprecedented times and the health department officials did not share their motivation for changing physician’s orders.”
Doctors Being Pressured to Add COVID-10 to Death Certificates
Daniel W. Erickson of Bakersfield, California, is a former emergency-room physician who co-owns, with his partner Dr. Artin Massih, Accelerated Urgent Care in Bakersfield. Watching the news in China in January, they knew the virus was on its way. They ordered many COVID-19 tests because they knew they would need them. They tested thousands of people, and discovered for themselves what epidemiologists around the world are now saying: COVID-19 came here earlier than previously believed, is more ubiquitous, and ultimately for the general population less deadly than we thought.
"When someone dies in this country right now they’re not talking about the high blood pressure, the diabetes, the stroke. They say they died from COVID. We’ve been to hundreds of autopsies. You don’t talk about one thing, you talk about comorbidities. COVID was part of it, it is not the reason they died folks. When I’m writing up my death report I’m being pressured to add COVID.
Why is that? Why are we being pressured to add COVID? To maybe increase the numbers, and make it look a little bit worse than it is. We’re being pressured in-house to add COVID to the diagnostic list when we think it has nothing to do with the actual cause of death. The actual cause of death was not COVID, but it’s being reported as one of the disease processes and being added to the death list. COVID didn’t kill them, 25 years of tobacco use killed."
The White House Coronavirus Task Force Confirms it is Inflating COVID-19 Deaths
On 7 April 2020, confirmation that the US was inflating the COVID-19 death toll came from a surprising source – the White House. During a press briefing, Dr Deborah Birx, response coordinator for the White House Coronavirus Task Force, told reporters the US has "taken a very liberal approach to mortality."
"There are other countries," said Birx, "that if you had a pre-existing condition and let’s say the virus caused you to go to the ICU and then have a heart or kidney problem — some countries are recording that as a heart issue or a kidney issue and not a COVID-19 death."
As they should.
But that's not how it now works in America, explained Birx, where "the intent is, right now, that those — if someone dies with COVID-19, we are counting that as a COVID-19 death."
 Deborah Birx proudly admits non-COVID-19 deaths are being counted as COVID-19 deaths in the US.
Deborah Birx proudly admits non-COVID-19 deaths are being counted as COVID-19 deaths in the US.
When a reporter queried the validity of this approach, Birx fumbled for a coherent response, leading none other than Dr Anthony S. Fauci to chime in. Fauci is another lead member of the White House Coronavirus Task Force and, if you are to believe the lavish media hype, one of the world’s most respected experts on infectious disease.
As Part 1 of this series explained, Fauci – in 2014 and 2019, as head of the NIAID - endorsed $7.4 million dollars of grants so that China’s Wuhan Institute of Virology could manipulate bat coronaviruses and make them even more virulent.
Here’s what this ‘respected expert’ had to say in defence of the COVID-19 counting strategy:
“I think there’s so much focus now on coronavirus that … No, I can’t imagine if someone comes in with coronavirus, goes to an ICU, and they have an underlying heart condition and they die — they’re going to say, “Cause of death: heart attack.” I — I cannot see that — that happening. So I don’t think it’s going to be a problem.”
Fauci openly admits that, thanks to the current COVID-19 hysteria, there is every chance a heart disease patient who dies of a heart attack while also having a coronavirus infection will misleadingly be listed as dying of COVID-19. And he also proudly admits he doesn’t see this as a problem.
Unbelievable.
 The dodgey Dr Fauci happily admits US authorities are ascribing deaths from other causes to COVID-19 – and sees absolutely nothing wrong with this highly misleading statistical chicanery.
The dodgey Dr Fauci happily admits US authorities are ascribing deaths from other causes to COVID-19 – and sees absolutely nothing wrong with this highly misleading statistical chicanery.
More People are Dying - But Not From What You've Been Told
If deaths from other causes are being erroneously listed as COVID-19 deaths, but the overall mortality rate remains the same, then we know something smelly is going on. It would tell us authorities have been shuffling the figures around, transferring deaths from other causes into the COVID-19 category, leaving overall mortality unchanged.
But if overall death rates in affected countries are significantly above average for this time of year, then it would suggest COVID-19 really is an unusually virulent and deadly 'pandemic.'
At first glance, this would seem to be the case.
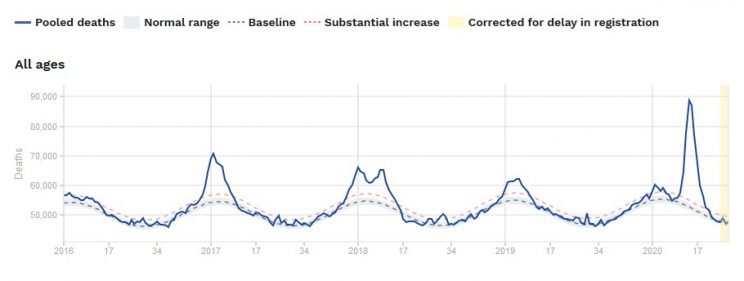
The graphs at this page contain overall mortality rates for various age groups from the start of 2016 and up to week 28 of 2020 (as of this writing), using data from 24 participating countries: Austria, Belgium, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Luxembourg, Malta, Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, UK (England, Northern Ireland, Scotland), Wales).
You’ll note that group includes Italy, Spain and the UK, all of which have reported a high prevalence of COVID-19. Italy and Spain especially have been the subject of countless doomsday media stories.
Here is the all-ages mortality graph. The solid blue line represents the combined actual death rate for the aforementioned countries. The broken grey line represents the baseline or ‘normal’ death rate, while the broken pink line represents a substantial increase in deaths from the baseline rate. Any time the death rate trajectory crosses above that broken pink line and stays elevated, it’s a signal for health authorities to sit up and take notice.
 Source: https://www.euromomo.eu/graphs-and-maps
Source: https://www.euromomo.eu/graphs-and-maps
Now, let’s take a closer look at the above graph, and what it tells about the current situation. The graph shows it was not until week 13 of 2020 that the overall weekly mortality rate for this group of countries passed the high of the 2017 winter.
It topped out at week 14, with 86,883 deaths, before rapidly falling back towards baseline by week 20.
As a quick aside, you’ll note overall mortality in these European countries reliably peaks during the height of the Northern Hemisphere winter – I’ll discuss the significance of this another time, along with how we can use this information to safeguard our health. Suffice to say for now that winter is the unhealthiest and deadliest time of year no matter what hemisphere you live in.
The graph above shows a higher spike in deaths for 2020 compared to recent years, albeit a relatively short-lived one. It also shows that the death rate began to rise above baseline in late 2019, just as it had done in previous years. However, by week 8 of 2020, overall mortality in Europe had returned to baseline. It then began to rise again, reaching the “substantial increase” threshold in week 11, before rapidly rising to produce the prominent spike visible to the right of the graph.
Now … to help place this all in better perspective, the cumulative death toll of the 2020 spike – during the periods it breached then returned to the “substantial increase” threshold (weeks 11-20) – was 677,328 people.
Let’s compare this to the spike of 2017-2018. In this winter, the “substantial increase” threshold was broached in week 49 of 2017 and revisited in week 15 of 2018. Total deaths during that period were 1,156,578.
The European COVID-19 ‘pandemic’ of 2020 has not claimed as many lives as the excess winter mortality of 2017-2018. Even if we include the earlier brief spike of 2020 (weeks 1-5) that occurred before COVID-19 is assumed to have reached Europe, the 2020 total rises to only 971,908.
Compared to the 2017-2018 death rate, the 2020 winter – which has been marked by unprecedented hysteria and a global house arrest campaign – suddenly doesn’t seem so lethal after all.
Supporters of all things big government, of course, already have their retort to this observation:
“Yeah, but if it weren’t for the lockdown, the death toll would have been much worse!”
There is little-to-no evidence the lockdown has saved lives, and mounting evidence to show it has increased deaths from other causes.
Based on a broad array of scientific data, non-profit Just Facts computed the anxiety created by reactions to COVID-19 — such as stay-at-home orders, business shutdowns, media exaggerations, and legitimate concerns about the virus — will destroy at least seven times more years of human life than can possibly be saved by lockdowns to control the spread of the disease. This figure is a bare minimum, and the actual one is likely more than 90 times greater.
The Just Facts study was reviewed by Joseph P. Damore, Jr., M.D., who concluded: “This research is engaging and thoroughly answers the question about the cure being worse than the disease.” Damore is a certified diplomate with the American Board of Psychiatry and Neurology, an assistant professor of psychiatry at the Weill Medical College of Cornell University, an assistant attending psychiatrist at New York Presbyterian Hospital, and an adjunct professor in the Department of Behavioral Sciences and Leadership at the U.S. Military Academy.
To gain further insight into the stupidity of the lockdown, let’s take a closer look at what is currently happening with deaths from other causes around the world.
When the Cure is Worse than the Disease
The figures in the mortality graph above, it bears reminding, are for overall mortality. They don’t tell us exactly how many people died of COVID-19 – or any other disease. And even if they did contain a breakdown of individual cause of death data, we know the COVID-19 death figures are suspect, because authorities have been employing numerous methods to inflate them.
We also know the COVID-19 hysteria has had other profound effects on health behaviour and resultant mortality. All around the world, for example, hospital emergency departments are reporting significant declines in admissions from non-COVID-19 causes.
Despite endless alarmist media reports of overloaded hospitals and health systems “on the brink of collapse,” a recent New York Times article by Harlan M. Krumholz, M.D. reported:
“The hospitals are eerily quiet, except for Covid-19.”
“I have heard this sentiment from fellow doctors across the United States and in many other countries,” says Krumholz, professor of medicine at Yale and director of the Yale New Haven Hospital Center for Outcomes Research and Evaluation. “We are all asking: Where are all the patients with heart attacks and stroke? They are missing from our hospitals.”
"What is striking," continues Krumholz, "is that many of the emergencies have disappeared. Heart attack and stroke teams, always poised to rush in and save lives, are mostly idle. This is not just at my hospital. My fellow cardiologists have shared with me that their cardiology consultations have shrunk, except those related to Covid-19. In an informal Twitter poll by @angioplastyorg, an online community of cardiologists, almost half of the respondents reported that they are seeing a 40 percent to 60 percent reduction in admissions for heart attacks; about 20 percent reported more than a 60 percent reduction.”
Rest assured: People are still suffering heart attacks and strokes, not to mention burst appendices, diabetic complications, and other life-threatening ailments. But, alarmingly, many have stopped presenting to emergency wards for medical help since COVID-19 paranoia took over.
Here in Australia, where the COVID-19 hysteria is beyond absurd considering the country’s small population and seasonal immunity advantage, a 29 April 2020 News.com.au story revealed:
"Emergency departments of major hospitals have been virtually deserted at times in recent weeks as people stay away during the coronavirus lockdown.”
Waiting times at hospitals have been slashed, doctors told News.com.au, as people stay at home for fear of being near COVID-19-infected people.
A similar scenario has unfolded in the UK. As patients stayed away from hospitals in droves, a 9 May 2020 report by the Guardian indicated an extra 8,000 people had died in their own homes since the start of the ‘pandemic’ than in normal times. Of that total, 80% died of conditions unrelated to COVID-19, according to their death certificates. Doctors’ leaders have warned that fears of the virus and de-prioritisation of non-coronavirus patients were taking a deadly toll.
The data showed 8,196 more deaths at home in England, Wales and Scotland compared with the five-year average for the same time of year, including 6,546 non-COVID deaths.
Doctors’ leaders have warned that some sick people are too scared to go to hospital and are aware much of the usual NHS care had been suspended because of COVID-19. “These figures underline that the devastation wrought by Covid-19 spreads far beyond the immediate effects of the illness itself,” said Dr Chaand Nagpaul, the council chair of the British Medical Association.
“While all parts of the NHS have rallied round in a bid to meet the immediate rocketing demand caused by the pandemic, more than half of doctors in a recent BMA survey have told us that this is worsening the care of non-Covid patients.”
He cited a fall in emergency department visits of up to 50% and a drop by half of patients attending hospitals with heart attacks.
“Referrals from GPs are not being accepted unless for serious medical conditions and routine investigations to aid diagnosis are not available in many cases. This means many ill patients are not getting the care they so desperately need now – and crucially, risking their conditions getting worse and with some even dying as a result,” Nagpaul added.
Italy: 11,600 Extra Non-COVID-19 Deaths in Just Over a Month
In the period between February 20 - when it recorded its first COVID-19 death - and the end of March, 90,946 people died of all causes in Italy. The average figure for that window is 65,592.
Of the 25,354 difference, about 54 per cent have been identified by health authorities as being caused by COVID-19, leaving about 11,600 other deaths unexplained.
Over the February 20 to March 31 period, 6,238 lost their lives in the hard-hit town of Bergamo compared to the usual 1,180. Only 2,346 of the extra 5,058 deaths were directly tied to coronavirus.
The Sydney Morning Herald claimed "The sharp difference suggests the true coronavirus death toll is much higher than [Italy's] present 29,079," but did not explain how it arrived at this suggestion. The paper failed to discuss the well-documented observation that, as in many other countries, Italians had been shying away from emergency wards, even when suffering heart attacks and strokes.
When the World Collectively Loses its Mind
These observations are being confirmed in medical journals by researchers all around the world.
From a quick internet search, I was able to retrieve published studies and journal letters showing the COVID-19 hysteria has, on average, slashed the number of admissions for cardiovascular emergencies by 40-50% in the USA, UK, Italy, Spain, Austria, Argentina, Canada, France and Norway[1-11].
One of the Italian reports, headed by researchers from the Italian Society of Cardiology, compared admissions for acute myocardial infarction (a.k.a. heart attack due to coronary heart disease) at Italian coronary care units throughout a 1 week period during the COVID-19 outbreak. They found a 49% reduction in admissions for AMI compared with the equivalent week in 2019. Not only were admissions for AMI significantly reduced, but there was a parallel increase in fatality and complication rates. "This constitutes a serious social issue," noted the researchers, "demanding attention by the scientific and healthcare communities and public regulatory agencies."
You bet it does. It’s a pretty lucid indicator that the COVID-19 scare campaign has gone way too far when people start telling themselves, “yep, I’ll take my chances on surviving this life-threatening heart attack at home, but no way am I going to hospital where I might catch a novel strain of flu!”
Over in Spain, researchers gathered data from 73 cardiology units throughout the country’s 17 autonomous regions. They found a "very significant decrease" in the number of diagnostic procedures (–56%) in coronary units during the outbreak compared to immediately prior. Emergency procedures for myocardial infarction and non-coronary heart disease declined by 40% and 81%, respectively. The Spanish researchers called upon health and scientific authorities to impress upon people that those with heart attack symptoms should "proceed with no delay” to access medical help and receive the appropriate emergency treatment.
After observing a 40% decline in the number of patients admitted for acute coronary syndrome, Austrian researchers estimated 275 ACS patients went untreated in March 2020. Based on data showing that the cardiovascular mortality of untreated ACS patients might be as high as 40%, this meant a likely 110 additional ACS deaths during this time frame. The researchers correctly noted this excess “is very alarming,” particularly when considering the official number of COVID-related deaths by March 26 in Austria was only 86.
Keep in mind this only represents deaths from ACS, not myocardial infarction, stroke and the multitude of other non-CVD medical emergencies that went unattended.
Concerned doctors from Hong Kong reported that, after the city's hospitals began instituting emergency infection protocols to contain COVID-19, patients were seeking medical assistance later in the course of their heart attack. This delay in seeking emergency treatment not only increases the likelihood of death but, if the patient survives, it increases the likelihood and severity of complications.
French researchers reported a similar phenomenon with ACS patients in France.
Note to World: Grow a Brain, For Chrissakes
I must say that, even after 52 years of observing what an incredibly irrational, gullible and self-destructive pack of twats Homo sapiens largely are, these observations absolutely stun me. It is truly astounding to think that anyone, upon experiencing the ominous signs of an impending heart attack or stroke, would sit there and think to themselves:
“Holy shit, I think I’m having a heart attack – call an ambulance! No wait, I might catch the coronavirus at the hospital! Nah, forget that – I’d rather stay home and die! At least that way, I won’t get coronavirus!”
Fuck. Me.
I mean seriously, what the hell is wrong with people?
To all you geniuses who would rather stare down an untreated heart attack or stroke, rather than possibly catch a far less deadly flu virus, let me ask you something:
When your coffin is being lowered into the ground, do you really think that – instead of sobbing and crying – your loved ones will instead be smiling, high-fiving each other, and proudly boasting “at least he didn’t catch the coronavirus! What a legend!” … ?
Here’s some valuable health advice for you, completely free of charge:
A heart attack or stroke is much, much more likely to kill you than COVID-19. Especially if you do not even have COVID-19. If you are experiencing symptoms suggestive of a coronary or cerebral event, CALL AN AMBULANCE OR GET YOUR DUMB ASS DOWN TO YOUR LOCAL EMERGENCY WARD IMMEDIATELY.
And while you’re at it, stop uncritically swallowing the egregious bullshit emanating from your dodgey governments and mainstream media outlets.
You can thank me later.
What is especially worrying about all this is that, according to IQ testing, Italy and Hong Kong are among the most intelligent countries in the world. If this is how the world’s smartest populations respond to a bullshit health scare, then I suspect humankind is well and truly fucked.
Using COVID-19 to Kill Off More of those Pesky Poor People
Thanks to the COVID-19 lockdowns, tuberculosis programs around the world have suffered shutdowns. Researchers estimate this disruption to tuberculosis services could lead to as many as 6.3 million additional cases of TB and an extra 1.4 million deaths worldwide over the next five years.
This would represent an 11 per cent increase in the number of TB cases between 2020 and 2025 and it would take the number of cases back to the levels they were in 2013.
Gee, where are the world-saving billions of the Clinton and Bill and Melinda Gates Foundations when the world’s poor really need them?
Disruption from the COVID-19 pandemic could also double deaths from malaria and erase 20 years of progress by anti-malaria campaigns.
Modelling by the World Health Organization has predicted that deaths in sub-Saharan Africa might reach almost 770,000 this year if the distribution of medicines and mosquito nets is halted.
The WHO urged countries to not overlook malaria during the new coronavirus pandemic and “do their utmost to safely maintain these essential malaria control services”.
Perhaps the WHO itself could aid this noble outcome by ceasing and desisting with the absurdly alarmist COVID-19 bullshit?
Just a thought.
By the way, I won’t start banging on about eugenics and world population reduction, lest those allergic to ‘conspiracy theories’ start breaking out in severe, itchy red rashes. That would be most embarrassing if they are reading this in public. All I will say here is if you’re one of the world’s oligarchical billionaires who harbours an obsession with overpopulation (as many of them do), then you’re probably sporting a very smug, sinister smile right now.
After all, the countries worst affected by tuberculosis and malaria are the most densely populated and/or poorest countries.
Who needs all those impoverished, starving people who are too poor to buy your bullshit software and consumer goods, right?
If the WHO and the world’s self-professed billionaire humanitarians really cared about the world’s poor, they would call an end to this COVID-19 charade pronto. Of course, they have no intention of doing so, because the COVID-19 fear campaign is proving itself to be the perfect Trojan Horse for enacting multiple nefarious agendas, none of which have the best interest of the common person at heart, let alone the world’s underprivileged and undernourished.
Driving People to Kill Themselves via Social Isolation and Unemployment. Gee, What a Great ‘Health’ Strategy!
According to Worldometer, as of this writing, there have been 655,201 deaths assigned to COVID-19 around the world. Just how many of those deaths were truly caused by COVID-19 is anyone’s guess, because we know officials have been wildly inflating the figures.
Meanwhile, as of this writing, there have been 614,965 deaths by suicide globally so far in 2020.
There have also been 1,434,318 deaths caused by alcohol so far this year.
Just how many of those suicides and alcohol-related deaths are attributable to the COVID-19 paranoia is yet to be ascertained.
What we do know is that the lockdown has led to skyrocketing unemployment levels, and past research shows increased unemployment is associated with a rising death toll from substance abuse and suicide.
In regards to suicide, doctors and counsellors on the ground are confirming what many of us fully expected: The COVID-19 hysteria and concomitant lockdown is driving more people to kill themselves.
During March 2020, Lifeline's US Disaster Distress Helpline saw a 338 percent increase in call volume compared with February 2020.
The Didi Hirsch Suicide Prevention Crisis Line, a major member of the US National Suicide Prevention Lifeline, received more than 1,500 calls about the coronavirus in March - 75 times more than the previous month.
Doctors in Northern California say they have seen more deaths from suicide than they’ve seen from the coronavirus during the pandemic.
“The numbers are unprecedented,” Dr Michael deBoisblanc of John Muir Medical Center in Walnut Creek, told ABC 7 News.
"We've never seen numbers like this, in such a short period of time," he said. "I mean we've seen a year's worth of suicide attempts in the last four weeks."
DeBoisblanc said he believes it’s time for California officials to end the stay-at-home order and let people back out into their communities.
Kacey Hansen, who has worked as a trauma nurse at the Center for 33 years, is worried because not only are they seeing more suicide attempts, she says they are not able to save as many patients as usual.
"What I have seen recently, I have never seen before," Hansen said. "I have never seen so much intentional injury."
"They intend to die," Hansen said. "Sometimes, people will make what we call a 'gesture'. It's a cry for help. We're just seeing something a little different than that right now. It's upsetting."
Hansen and deBoisblanc say they are seeing mostly young adults die by suicide. They are worried about the stress that isolation and job loss can bring as this quarantine continues.
Confirming that the cure is far worse than the disease, more people died of suicide in a single Tennessee county in the last week of March than of COVID-19 across the entire state.
Knox County Regional Forensic Center examined nine suspected suicides in under 48 hours, according to Knox County Mayor Glenn Jacobs. State Department of Health data showed six people died of COVID-19 in Tennessee during the same week.
"Is what we are doing now really the best approach? How can we respond to COVID-19 in a way that keeps our economy intact, keeps people employed, and empowers our people with a feeling of hope and optimism, not desperation and despair?” Jacobs asked.
“Thus far, our reaction to COVID-19 has been to sacrifice the global economy,” Jacobs said. “The truth is: a sick economy produces sick people.”
In late May, Arizona's Pima County Health Department also reported a spike in suicide rates over recent months. The sharpest increase was 15 suicides within a 14-day span during March.
According to estimates released by Well Being Trust (WBT) and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, the COVID-19 phenomenon could lead to 75,000 additional deaths from alcohol and drug misuse and suicide.
The research brief notes that three factors, already at work, are exacerbating "deaths of despair": unprecedented economic failure paired with massive unemployment, mandated social isolation for months and possible residual isolation for years, and uncertainty caused by the sudden emergence of a previously unknown microbe.
500+ Doctors Write to Trump, Calling Lockdown a “Mass Casualty Incident”
The situation is so dire that over 500 physicians signed a letter, dated 19 May 2020, to President Donald Trump pleading him to end the shutdown, which they called a “mass casualty incident.”
The signatories warned that as every last medical resource is devoted to the pandemic, many Americans who would be at a high priority triage level had they presented for medical help are instead going untreated.
“These include 150,000 Americans per month who would have had a new cancer detected through routine screening that hasn’t happened, millions who have missed routine dental care to fix problems strongly linked to heart disease/death, and preventable cases of stroke, heart attack, and child abuse.”
“Suicide hotline phone calls have increased 600%,” the doctors also noted. “Liquor sales have increased 300-600%, cigarettes sales have increased, rent has gone unpaid, family relationships have become frayed, and millions of well-child check-ups have been missed.”
Ironically, Trump himself warned back in March that the lockdown would cause “suicide by the thousands,” only to be pooh-poohed by his own CDC and mocked by the establishment-run media, which has been rabidly obsessed with undermining his Presidency from the moment he was elected.
Suicides Rising in UK Too
Over in the UK, police chiefs also reported a rise in suicides and suicide attempts within weeks of the commencement of Britain's lockdown.
Refuge, the UK's largest domestic abuse charity, said calls to its National Domestic Abuse Helpline had risen by 25 per cent during the week commencing 30 March, at the start of the lockdown imposed by the Prime Minister.
Meanwhile, hits to the national domestic abuse website www.nationaldahelpline.org.uk increased by 150% during the initial stages of the lockdown.
Hysterical Bullshit Kills
The journal Brain, Behavior, and Immunity recently published a paper by Indian researchers Vikram Thakura and Anu Jain titled "COVID 2019-suicides: A global psychological pandemic." The article cites a number of potential mechanisms by which COVID-19 is driving people to kill themselves - and others:
- Social Isolation/distancing
- The economic recession caused by the worldwide lockdown
- Stress, anxiety and pressure in medical healthcare professionals
- Social discrimination
The article cites a number of disturbing cases induced by the insane lockdown.
In India, where suicides have dramatically spiked during the lockdown, a 50-year-old man wrongly assumed his normal viral infection was COVID-19. He initially quarantined himself, but later committed suicide, as he was psychologically disturbed after reading about COVID-19-related deaths in the newspaper.
In April, a 65-year-old Indian woman committed suicide citing fear she would infect her daughters coming to see her the next morning. Officials said she had no COVID symptoms or history – her fear was an illusion. The woman had been depressed since the death of her husband last year.
In Chicago, Patrick Jesernik, 54, shot Cheryl Schriefer, 59, before shooting himself. The impetus for the murder-suicide was Jesernik's belief the two of them were infected with COVID-19. An autopsy determined that both Jesernik and Schriefer were negative for the virus.
In March, 34-year-old nurse Daniella Trezzi, who worked in the COVID-19 intensive care ward of San Gerardo hospital at Monza, near Milan, learned she had been infected with the virus. Distraught at the idea she could have spread the coronavirus to others, and facing the relentless working conditions at a hospital in the epicenter of the pandemic in Europe, Trezzi tragically committed suicide.
Also in March, a 49-year-old nurse who worked in the COVID-19 ward of Jesolo hospital committed suicide, throwing herself into the Piave river in Cortellazzo, in the region of Venice. The nurse lived alone and was at home for two days with a fever and was awaiting the results of a COVID-19 test, when she took her own life.
UK girl Emily Owen, 19, died in late March after feeling ‘she could no longer cope’ with impending lockdown measures due to COVID-19, her family said. After attempting suicide, she was rushed into critical care but failed to regain consciousness. Her family said she had been deeply affected by the global pandemic and had spoken of her wish to help people with mental illnesses navigate their own way through the isolation measures.
 Emily Owen: A beautiful and, by all accounts, community-minded young lady driven to suicide by the cynical COVID-19 hysteria.
Emily Owen: A beautiful and, by all accounts, community-minded young lady driven to suicide by the cynical COVID-19 hysteria.
In February, a Chinese student living in Saudi Arabia committed suicide after being quarantined in hospital on suspicion of being infected with COVID-19. The patient was placed in a completely closed isolation room, but threw himself out of the room after removing the window’s safety button. Subsequent laboratory results showed he was not infected with the virus.
The Unlucky Country Gets Even Unluckier
As a country with massive mental health issues and a fragile economy precariously relying upon the good fortunes of the mining industry and continued stimulation of an unsustainable housing bubble, a lockdown was the last thing Australia needed.
Despite all its self-congratulatory bollocks about being “the lucky country” and the heavily promoted image of Australians as laidback, happy-go-lucky people, the truth about Australia is that it is one of the most debt-ridden, drug-addled, depressed, anxious and highly strung countries on the planet.
A 2015 World Health Organization Report found Australia shared the second-highest rate of depression alongside the US and Estonia (Ukraine had the highest rate). Australia had the third-highest rate of anxiety, behind Brazil and New Zealand.
Thanks to its highly superficial, consumerist culture and notoriously steep cost of living, Australia has the second-highest rate of household debt in the world.
Other Down Under ‘achievements’ the Australian government and media prefer not to highlight are the world’s eleventh-highest incidence of reported rape and a sickeningly high rate of pedophilia.
In a comparison of 22 countries for which data was available, Australia ranked second only to South Africa for the prevalence of child sexual abuse of females. For sexual abuse of male children, Australia ranked sixth behind South Africa, Jordan, Tanzania, Israel and Spain[12].
As Australians struggle to afford overpriced houses, cars and utility costs that are among the highest in the world, and deal with alarming rates of sexual predation, they are downing world-beating quantities of prescription and illicit drugs.
Australia is the world’s third-highest consumer of antidepressant drugs, behind the US and Iceland.
Australians and New Zealanders are the world’s highest per capita consumers of cocaine and ecstasy, and rank second only to North Americans for per capita use of cannabis, amphetamines and pharmaceutical stimulants[13]. North Americans and Australians/New Zealanders also share the world’s highest per capita rates of opioid use (3.6% vs 3.3%, respectively)[14].
Suffice to say, Australia is mentally ill-equipped to handle the challenges of a lockdown. Racist Aussies presume to tell Indigenous Australians to just “get over it” and casually shake off hundreds of years of mistreatment, racism and cultural decimation. Meanwhile, during the height of the lockdown, Anglo- and European-Australians were completely losing their shit in supermarkets simply because they were only allowed two cans of tuna or two packs of pasta per visit. Instead of simply returning the next day to buy 2 more of the same item, Aussie logic instead dictated they throw an unbecoming tantrum in the middle of a busy supermarket. Sometimes their tantrums turned violent, with young staff being physically assaulted, fist fights among customers, and knives even pulled in order to secure the last pack of toilet paper.
Fucking brilliant.
New research suggests Australians are going to pay dearly for the malfeasance of their leaders and their country’s widespread stupidity and gullibility.
According to researchers from Sydney University’s Brain and Mind Center, a spike in suicides triggered by COVID-19 lockdowns is expected to exceed deaths from the actual virus by a factor of ten in Australia.
Australia’s suicide rate could surge by up to 50 per cent as the mental health impacts of the economic fallout from the lockdowns take hold.
The Brain and Mind Centre's modelling forecast the financial and psychological toll could result in an extra 750 to 1,500 suicides a year, with fears Indigenous and multicultural communities are among those at greatest risk. The modelling was based on outcomes observed during the 2009 Global Financial Crisis, 1997 Asian Financial Crisis and the 1930s Great Depression.
These figures dwarf the 161 deaths ascribed to COVID-19 in Australia so far.
As an isolated country with a very small population (a mere 25 million people on a land mass slightly larger than China), Australia was never at great risk of suffering a high number of COVID-19-related deaths. It is also important to note that, due to its Southern Hemisphere location, Australians were nearing the end of summer when the virus peaked. This meant that, unlike their Northern Hemisphere peers, Australians’ natural immunity and infection resistance were at their highest levels, in no small part due to a seasonal peak in sunlight exposure and hence vitamin D status.
The Australian response to COVID-19, which has involved harsh fines for breaching the arbitrary social distancing guidelines, border closures and an international travel ban, is a textbook classic example of wanton authoritarian overkill. With overseas travel off limits to all but those leaving for work or returning to their foreign home, Australia has effectively been relegated to a more urbanized version of what it was in the late 1700s:
A giant prison island.
A much more sensible and far less destructive strategy would have been to simply educate the Australian public on the importance of personal hygiene. In a land where many people still think bidets are for “pooftahs” and that washing one’s hands after going to the toilet is a time-consuming inconvenience, basic hygiene education would be of infinitely more use than wearing surgical masks and screaming racial obscenities at innocent Asian folks. I’ve lost count at the number of times over the years I’ve watched men walk out of public toilets without washing their hands (female family and friends tell me the situation is no better in ladies’ toilets), and I am stunned by the number of Australians too dumb or indifferent to cover their mouths when they cough or sneeze in public. Instead of using COVID-19 to accelerate Australia’s transition from nanny state to full-blown police state, why not just start teaching Australians good manners and hygiene from a young age?
I guess the answer is because that would make too much sense.
And it would also fail to fulfil one of the key purposes of the COVID-19 sham, which is for governments and their elite masters to impose ever greater control and surveillance over us mere plebs.
We are undergoing a cruel social experiment on a global scale, and our sadistic elite knew full well what would transpire from this experiment. As they sip top shelf wines and count the extra money their lockdown-immune businesses raked in during the ‘pandemic’, people around the world are suffering the predictable physical and mental effects of forced isolation.
In the next article, I’ll discuss the research showing social isolation is so harmful that some countries have even banned solitary confinement from their prisons.
Ciao,
Anthony.
PLEASE NOTE: If you are experiencing thoughts of self-harm or suicide, please do not suffer in silence. Please reach out to a counsellor or crisis helpline. Because of my global readership, it is impossible for me to provide help hotline numbers for every country, but a quick internet search for suicide hotlines should retrieve such numbers for your locality.
Please avoid antidepressant drugs as they have been shown to increase the risk of suicide in all ages (not just under 25s as the official propaganda claims). The suicide risk of antidepressants is especially pronounced during the first month of use, after dosage changes and in the first month after cessation of use. If you are already taking antidepressants and wish to stop, do not do so suddenly – taper down your dose and let your family, friends and doctor/s know what you are doing.
If you are experiencing symptoms of a serious medical condition, call an ambulance or the appropriate emergency number for your location, or present yourself to an emergency ward as soon as possible. COVID-19 is highly unlikely to kill you, but an untreated heart attack or stroke can easily prove fatal.
If You Enjoyed this Article, Please Consider Sending a Tip
Donate with Crypto
References
- Solomon MD, et al. The Covid-19 Pandemic and the Incidence of Acute Myocardial Infarction. New England Journal of Medicine, 2020; DOI:10.1056/NEJMc2009166.
- Garcia S, et al. Reduction in ST-Segment Elevation Cardiac Catheterization Laboratory Activations inthe United States during COVID-19 Pandemic. Journal of the American College of Cardiology, https://doi.org/10.1016/j.jacc.2020.04.011.
- Mafham MM, et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet, 2020; S0140-6736 (20): 31356-31358.
- Vecchio S, et al. Impatto della pandemia COVID-19 sui ricoveri per sindrome coronarica acuta: revisione della letteratura ed esperienza monocentrica. Giornale Italiano di Cardiologia, 2020; 21 (7): 502-508.
- Rodríguez-Leor et al. Impacto de la pandemia de COVID-19 sobre la actividad asistencial en cardiología intervencionista en España. REC Interventional Cardiology, 2020; 2 (2): 82-89.
- Metzler, B, et al. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: the pandemic response causes cardiac collateral damage. European Heart Journal, Apr, 2020; 41, 1852–185.
- Bozovich GE, et al. Daño colateral de la pandemia por COVID-19 en centros privados de salud de Argentina. Medicina, 2020; 80 (Suppl. III): 37-41.
- Bullrich MBB, et al. COVID-19: Stroke Admissions, Emergency Department Visits, and Prevention Clinic Referrals. Canadian Journal of Neurological Sciences, 2020; 00: 1–4.
- Hauguel‑Moreau M, et al. Impact of Coronavirus Disease 2019 outbreak on acute coronary syndrome admissions: four weeks to reverse the trend. Journal of Thrombosis and Thrombolysis, 2020; https://doi.org/10.1007/s11239-020-02201-9.
- Lantelme P, et al. Worrying decrease in hospital admissions for myocardial infarction during the COVID-19 pandemic. Archives of Cardiovascular Disease, 2020; 113: 443-447.
- Saxhaug Kristoffersen E, et al. Effect of COVID-19 pandemic on stroke admission rates in a Norwegian population. Acta Neurologica Scandinavica, 2020; doi:10.1111/ane.13307
- Pereda M, et al. The prevalence of child sexual abuse in community and student samples: A meta-analysis. Clinical Psychology Review, 2009; 29: 328–338.
- United Nations Office on Drugs and Crime. World Drug Report 2020 (United Nations publication, Sales No. E.20.XI.6): Tables 1 and 2, pages 43 and 44.
- Ibid: Page 15.
Global death toll from COVID-19, suicide and alcohol updated 28-07-2020.